
A Health Public Policy Nightmare
Vaccine spike antigen and mRNA persist for two months in lymph node germinal centers...

Immune imprinting, breadth of variant recognition and germinal center response in human SARS-CoV-2 infection and vaccination Cell. Published:January 24, 2022DOI:https://doi.org/10.1016/j.cell.2022.01.018
Highlights (per the journal)
Vaccination confers broader IgG binding of variant RBDs than SARS-CoV-2 infection
Imprinting from initial antigen exposures alters IgG responses to viral variants
Histology of mRNA vaccinee lymph nodes shows abundant germinal centers
Vaccine spike antigen and mRNA persist for weeks in lymph node germinal centers
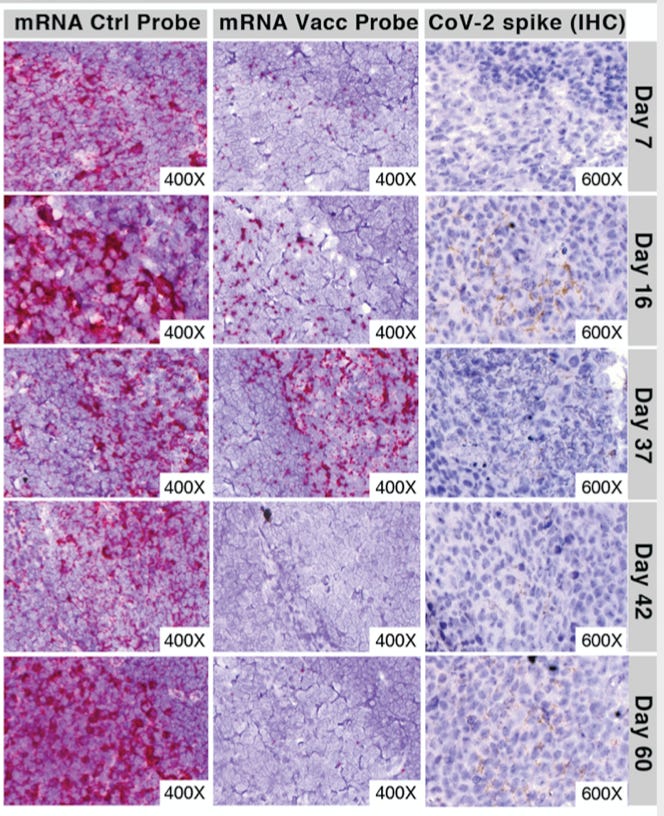
This study asserts that the mRNA and the spike protein produced persists for weeks in lymph node germinal centers in human patients. Immunohistochemical staining for spike antigen in mRNA vaccinated patient LNs varied between individuals, but showed abundant spike protein in germinal centers 16 days post-2nd dose, with spike antigen still present as late as 60 days post-2nd dose. Having worked with mRNA for decades, I can attest that this is highly unusual.
One very real hypothesis is that the substitution of pseudouridine for uridine to avoid the immune response is working so well that the mRNA is completely evading the normal clearance/degradation pathways. Hence, mRNA that is not being incorporated into cells at the injection site, is migrating to the lymph nodes (and throughout the body as the non-clinical Pfizer data suggest?) and continuing to express protein there. In this case, the cytotoxic protein antigen is spike. Spike protein can be detected for at least 2+ weeks after administration of dose. It did not appear that spike protein was tested for later than that, although the study is poorly worded in this regard. Nevertheless, abundant spike protein was detected after vaccination that continues for an indefinite time.
The spike protein, let’s review what it is and how it is being used (from the Daily Skeptic):
These new gene-based ‘vaccines’ are working in a completely novel way – nothing remotely resembling that of traditional vaccines. Given that pharmaceutical companies work competitively it was also somewhat of a surprise they took the same approach of targeting what has been termed the ‘spike protein’ of the SARS-CoV-2 virus.
This (spike) protein is nasty – sometimes being referred to as a ‘pathogenic protein’ – and is recognised as causing many of the awful pathologies associated with the disease of COVID-19. Logically you would inactivate or at least attenuate this nasty spike protein and develop a vaccine around the attenuated virus. But that’s not what was done. These ‘vaccines’ do not contain any of the offending virus at all but rather the gene sequence that causes the nasty spike protein to be made in the body. We have little idea how much of this nasty protein is produced or for how long it lasts after an injection of the gene sequence. Furthermore, stimulating the body’s own complex biological systems to produce the spike protein will mean that the amount of protein produced will vary from person to person. The idea is that the spike protein produced by the gene encoding it elicits a response by our immune system to produce antibodies directed against the spike. When the wild virus comes along and infects us the antibodies recognise the spike protein and attack it thus preventing its nasty effects. And it does, though as we have since learnt this approach isn’t very good at preventing infection or stopping its transmission. Are we perhaps clutching at straws too in claiming that these ‘vaccines’ are preventing serious disease and death? Have we not learnt anything over the past two years in treating Covid symptoms with conventional therapeutic drugs?
Knowing what we know about the spike protein in these vaccines, the study quantitatively measured spike protein levels in plasma after vaccination. This should have been characterized long ago, including prior to beginning human clinical trials.
That this has not been published or investigated more demonstrates the gross regulatory dereliction of duty by Pfizer, Biointech, Moderna, NIAID VRC and that whole crew. Using these vaccines, which include pseudouridine without fully understanding the implications and without the FDA requiring a complete pre-clinical toxicology regulatory package, including long-term follow-up, as is done with any other unique chemical or adjuvant additive is shocking. Then there is the novel use of the unique nano particles being used in these vaccines, which also were only marginally assessed, as shown by the Japanese Pfizer data.
Protein expression is not being turned off, because the immune response against the mRNA/pseudouridine complex is either not happening or is ineffective. It is clear that the mRNA/pseudouridine complex has a longer half-life than normal mRNA - by as long as 60 days. Normal mRNA breaks down within a few hours in the body. That this is lasting 60 days is unimaginable. The In either case, this is regulatory nightmare.
I do not know how to write this more strongly. This technology is immature. The WHO has approved six, more traditional vaccines, all of which the US government could license. These genetic vaccines are not the only option.
To note: The use of pseudouridine in these mRNA vaccines is not the only option. It has often been hypothesized that the reason Dr. Kariko added pseudouridine to the mRNA vaccine was to make an improvement to the original mRNA patents that I was an inventor on. An improvement to an existing patent allows commercialization of that patent. It is an old trick. Remember, that Curevac does not use pseudouridine in its formulation and it is not required or necessary for a significant immune response. In the next generation of mRNA vaccine experiments (hopefully done in an animal model), it is clear that the issues of adding pseudouridine need to be addressed prior to any more of these vaccines going into humans.
I know the following from the paper is long, but it is very important.
Prolonged detection of vaccine mRNA in LN GCs, and spike antigen in LN GCs and blood following SARS-CoV-2 mRNA vaccination
The biodistribution, quantity and persistence of vaccine mRNA and spike antigen after vaccination (with the Pfizer vaccine), and viral antigens after SARS-CoV-2 infection, are incompletely understood but are likely to be major determinants of immune responses. We performed in situ hybridization with control and SARS-CoV-2 vaccine mRNA-specific RNAScope probes in the core needle biopsies of the ipsilateral axillary LNs that were collected 7-60 days after 2nd dose of mRNA-1273 or BNT162b2 vaccination, and detected vaccine mRNA collected in the GCs of LNs on day 7, 16, and 37 post vaccination, with lower but still appreciable specific signal at day 60 (Figures 7A -7E). Only rare foci of vaccine mRNA were seen outside of GCs. Axillary LN core needle biopsie of non-vaccinees (n = 3) and COVID-19 patient specimens were negative for vaccine probe hybridization. Immunohistochemical staining for spike antigen in mRNA vaccinated patient LNs varied between individuals, but showed abundant spike protein in GCs 16 days post-2nd dose, with spike antigen still present as late as 60 days post-2nd dose. Spike antigen localized in a reticular pattern around the GC cells, similar to staining for follicular dendritic cell processes (Figure 7B). COVID-19 patient LNs showed lower quantities of spike antigen, but a rare GC had positive staining (Figure 7F). Immunohistochemical staining for N antigen in peribronchial LN secondary and primary follicles of COVID-19 patients (Figures 7F - 7I) was positive in 5 of the 7 patients, with a mean percentage of nucleocapsid-positive follicles of more than 25%.
Discussion One of the positive developments amid the global calamity of the SARS-CoV-2 pandemic has been the rapid design, production and deployment of a variety of vaccines, including remarkably effective mRNA vaccines encoding the viral spike (Baden et al., 2021; Polack et al., 2020). We find that BNT162b2 vaccination produces IgG responses to spike and RBD at concentrations as high as those of severely ill COVID-19 patients and follows a similar time course. Unlike infection, which stimulates robust but short-lived IgM and IgA responses, vaccination shows a pronounced bias for IgG production even at early time point
This Substack article has only skimmed the surface of the implications of this paper in terms of both the science and the malfeasance on the part of our government and pharmaceutical corporations. There is more to come on this issue.
To get to the full paper to download, click here.
Why Weren’t These Vaccines Put Through the Proper Safety Trials For Gene Technology, Asks a Former Pharmaceutical Research Scientist The Daily Skeptic 7 February 2022 by Dr. John D. Flack
This article by the daily skeptic does a great job at documenting that appropriate studies have not been done and even attempts to answer the question why:
Are we perhaps clutching at straws too in claiming that these ‘vaccines’ are preventing serious disease and death? Have we not learnt anything over the past two years in treating Covid symptoms with conventional therapeutic drugs?
Perhaps this has driven Big Pharma to pursue a new more profitable model based on protecting the healthy rather than treating the sick? Enter the era of the gene-based ‘vaccines’. The new technologies have had a long and difficult gestation period with several stillbirths. But perhaps their time had come with the ‘unprecedented’ virus from the East. A declared worldwide health emergency demanded a technological response, and it was there in waiting. But have we been blinded and duped by technology and lost sight of the end game of providing safe and effective medicines? Was it a judicious use of the PCR, rapid antigen test technology and information APP technology to drive the test and trace fiasco?
Was the gene technology ready to be used in a mass world-wide vaccination programme without a thorough examination of the potential problems of short- and long-term safety of this previously untested technology?
In my view, technocracy has trumped the sound principles, established over decades and centuries, of basic medical practice, immunology, virology, pharmaceutical sciences and public health generally. In the process, political democracy, personal freedoms, free speech and choice have been dangerously sidelined and even censored.
First of all, thank you very much Dr. Malone for your wisdom and your expertise during this vaccine nightmare. I have been following you consistently since you became public and if I could give you a medal for bravery I would certainly do it. I am a physician assistant and I am not vaccinated. Prior to becoming a PA I worked as a biochemist on the early development of the pneumococcus vaccine. I completely understand cytokine storm, chemotaxis, macrophage and mast cell migration in the lung as well as complement pathway immune response to pathogens in the lungs. In my scientific mind I can picture the lung damage that has happened to Covid patients as well as what has happened to me as I have long haulers. I had the alpha variant February 2020. I continue to see “Covid“ patients since the identification of the virus. I can say that I have definitely watched and examined the impact of this virus over the last two years. I have seen the symptoms decrease as the contagiousness of the virus increased and death decreases. But again that is the nature of most mutated viruses over a period of time as you well know. The delta variant acted out of line. I researched the molecule it seems that a component of acetic acid may have been substituted On one of the binding sites. Perhaps this could explain why Delta had made so many people very sick as I’m not sure that I could tolerate vinegar in my lungs as well! I question patients who say they’ve had Covid more than once as per your research you can continue to circulate the spike proteins for up to 15 months whether it is active or not. My observation thus far in the vaccinated patients is exactly what you stated in terms of spike population in lymph nodes. I have sent several patients for ultrasounds of “masses“ distributed in lymph node anatomical positions usually in the head and neck area including the cervical nodes and occipital and one in the axilla . So far four out of five patients over the last three months who had biopsies of these enlarged lymph nodes have been given the diagnosis of lymphoma. These are otherwise healthy individuals who were vaccinated by Moderna or Pfizer. I have not seen or read any further information about this with the exception of your latest article coming out of England. I can tell you that in the community I live in which is a retirement community people are dropping like flies! And I am sorry for those of you who are reading these comments if you have been vaccinated and are afraid to hear adverse reactions to the Covid vaccines. This is the epitome of the human experiment. This is criminal! I have been ostracized and nearly shunned from the medical community because I am not vaccinated and I refuse to be vaccinated not only because I researched it but also I had stage one Guillain-Barré syndrome following the flu vaccine 11 years ago. The most disgusting comment I have heard thus far is from some of my colleagues. When I challenged them about the adverse reactions to the Covid vaccines that they themselves are seeing in their own patients their response has been: “The sacrifice of a few benefits the many.” I call it the Fauci doctrine. It is becoming more and more difficult for me to continue to see patients who are experiencing adverse reactions to the Covid vaccines. I just don’t know what to say to them. I am forbidden to discuss the vaccines by my superiors. I don’t have your credentials or MD after my name I am simply a physician assistant who has been practicing for 36 years and never dreamt that as I am winding down the end of my career that it would be during a period of healthcare corruption. Keep doing what you’re doing, we need your voice.
If the body can't clear these protein spikes, then I'm concerned this could lead to autoimmunity.