
AMERICA – WE HAVE A PROBLEM
We are witnessing a cover-up of vast proportions and implications.


By: Brett Vance
Brett Vance is a former career Air Force fighter pilot, test pilot, and airline pilot who recently retired from his position as a test pilot in the Aircraft Certification Service with the Federal Aviation Administration. During his career, he accumulated over 7,500 flying hours, flew over 120 different aircraft, and earned ten type ratings in aircraft ranging in size from the B-777 to the Cessna 510. Primary military aircraft were the T-38, A-10, and the F-16.
Prologue
Astronaut and Mission Commander of Apollo 13, James A. Lovell, reported to Mission Control on 13Apr70, “Houston, we’ve had a problem” when announcing a Main Bus B Undervolt malfunction caused during an oxygen tank explosion. Most people know the story of incredible teamwork and courage that ended in the safe return of the crew following this near-catastrophic mission abort. Today’s lingo of that transmission is “Houston, we’ve got a problem,” and is generally associated with the appearance of a sudden unforeseen situation. It is also usually a huge understatement.

That’s the case now. However, just notifying Houston is not near enough. The whole of America needs to know what’s happening to our National Airspace System. Our NAS—the collection of systems and people that fly you safely from place to place—here in the U.S. is the safest on the planet…at least it was until now. While NASA was able to return three astronauts safely to earth and thus avert a potential catastrophe, the potential catastrophe facing our National Airspace System is similarly dire, but with vastly more terrifying consequences.
Under discussion here are the following topics that contribute to this problem. First, the departure from the industry, for a variety of reasons, of large numbers of highly-qualified and experienced commercial flight crews. Second, the effect of the covid shots and the mandates on flight safety since their rollout. Finally, and worst of all, the coverup.
Part 1 – Where is My Crew?
The first part of the problem with our NAS is the drawdown in the nation’s commercial pilot force. These are the folks that earn their living flying, many of whom are your airline pilots. You’ve all most likely heard of or personally experienced turmoil in flight schedules. And you think it’s what you’re told that weather or Air Traffic Control is to blame for this mess! That’s partially true, but you may have heard that crew availability is also to blame. The airlines will tell you that crews are just out of position and can’t get to where they need to be in a timely manner. What they are not telling you is that they just don’t have enough crews. So, what’s wrong with that? Just fess up and fix it. Right?

Obviously, it’s the companies’ job to properly staff the airline to accommodate what we call irregular operations. What happened…and why now? First, the argument is made that there was already a pilot shortage before the pandemic. Next, a look at the impact on staffing because of the COVID pandemic is warranted. With the initial rapid drop in demand for flying, airlines incentivized early retirements. Additionally, furloughs took their toll as people departed for other careers, never to return. As we then learned that the virus was not as severe as expected and had a very high survival rate, demand for air travel began to return, and return fast. With demand now at pre-pandemic levels or even higher, the airlines could not replace those departed crews. Next is the worst part of this equation—vaccine mandates. This collection of foolish decisions is surprising in the magnitude of its harmful effect.
Part 2 - The Covid Shot and the Mandates
By now everyone who is paying attention has realized that something is amiss with the COVID 19 gene therapy shots. You’ve probably seen reports of severe adverse reactions up to and including death, reports of people of all ages dying suddenly in their sleep, and athletes of both sexes at the peak of physical condition collapsing in practice or in competition. These conditions, we are learning, are not caused by the virus; rather, they are caused directly by the contents of the vials or because of a significantly weakened immune system from taking shot after shot

.There’s another cohort that we need to think about in case you are not aware. This group is in the aviation industry, and this article will focus on the cockpit crew in that aircraft that gets you safely where you want to go. Know that flight attendants, air traffic controllers, and support personnel are also affected; however, a problem with your pilots can lead to a disaster, killing you and maybe hundreds of other innocent passengers and even people on the ground. This article highlights those pilots.
We face a two-pronged dilemma, both of which must be addressed. First, the governments of the countries forcing flight crews to be “vaccinated” must immediately withdraw those mandates. Next, the pilots who took the shot and are adversely affected must be helped to reverse those ill effects.
Most of us are busy living our own lives and making ends meet. That means you’re probably not paying attention to this problem; and when you hear there is a problem, the properly-enquiring mind would want to know how big this problem really is and what this really means. Take a look at this excerpt from New Zealand’s Daily Examiner to get a feel for what we are all facing and how it was caused.
Excerpt from Airline Pilots Fight For Safety, For Themselves & Their Passengers
The US Federal Aviation Authority (FAA) is also extremely strict with its requirements for pilots. Specifically, title 14 of the Code of Federal Regulations §61.53 states that “no person who holds a medical certificate issued under part 67 of this chapter may act as pilot in command, or in any other capacity as a required pilot flight crewmember, while that person… [is] receiving treatment for a medical condition that results in the person being unable to meet the requirements for the medical certificate necessary for the pilot operation.”
In interpreting this provision, the Guide for Aviation Medical Examiners (AME) states, in reference to the issuance of medical certificates in the instance of use of pharmaceuticals as therapeutic medications for “Do Not Issue – Do Not Fly” orders, to include classes of medications or medications which:
“FDA (Food and Drug Administration) approved less than 12 months ago. The FAA generally requires at least one-year of post-marketing experience with a new drug before consideration for aeromedical certification purposes. This observation period allows time for uncommon, but aeromedically significant, adverse effects to manifest themselves….”
This portion of the regulations was highlighted in a letter issued to the FAA by a group of attorneys, medical doctors, and other experts on 15th December 2021, noting the serious adverse reactions to covid vaccines being experienced by pilots (including death) and asking for specific health checks on all vaccinated pilots.
The letter asks that all vaccinated pilots be medically flagged and:
“having said pilots undergo thorough medical re-examinations to include D-Dimer tests (to check for blood clotting problems), Troponin tests (to check for Troponin in the blood, which is a protein that is released when the heart muscle has been damaged), post-vaccination ECG analysis (also known as EKG, which checks the electrical signals which determine cardiac health), and cardiac MRI and PULS Test (to determine heart health).
According to the letter’s authors, inclusion of the cardiac MRI as a screening test for pilots is critical and referenced a recent study showed that using only ECG results and symptoms to screen patients resulted in a 7.4-fold under-diagnosing of actual myocarditis. The PULS Test is also important as an abstract published in the medical journal Circulation, entitled “Observational Findings of PULS Cardiac Test Findings for “Inflammatory Markers in Patients Receiving mRNA Vaccines”, found that “the mRNA vacs [vaccines] numerically increase … the markers IL-16, Fas, and HGF, all markers previously described by others for denoting inflammation on the endothelium and T cell infiltration of cardiac muscle”.
The letter’s authors also reference an affidavit filed in a US court earlier this year, where doctors including the cardiologist retained by the FAA and a Lieutenant Colonel in the US Army who is a flight surgeon, Aerospace Medicine Specialist, and an Aviation Officer Course & Mishap Training Specialist with a Master’s Degree in Public Health, concluded that
“the risk of “post-vaccination myocarditis was not trivial”
“that the “aviation population is comprised of individuals with demographics that the CDC and FDA established (on June 25, 2021) was at greatest risk for developing post-vaccination induced myocarditis”
“that the “unpredictable and potential serious complications thereof present an … unacceptable level of aeromedical risk,”
that “risk-stratification, screening and diagnostic testing is necessary for continued safety of flight,” and
that “immunizations with COVID vaccinations should be immediately suspended until further aviation specific studies can be conducted.”
It is worth noting that coincidental to the issuance of this letter to the FAA, NZ’s Ministry of Health issued an urgent letter to all primary healthcare providers and vaccinators. The letter admitted that incidences of vaccine-associated myocarditis and pericarditis have been under-reported in NZ and that the actual incidence, particularly for boosters, is not known. Instructions were also issued to include warnings on those serious side effects specifically, to those receiving the covid vaccines.
Clearly, serious vaccine-associated adverse reactions can be life-altering to those individuals who suffer them. However, the consequences for airline passengers if their pilots experience sudden effects are also devastating. The letter to the FAA continues and points out that
“… should the FAA fail to ground and medically de-certify all pilots who have received experimental and non-FDA approved COVID-19 vaccines in accordance with CFR §65.13 and related Guidance which require this result – and bar reinstatement of such pilots until such time as they can show aeromedically acceptable D-Dimer, Troponin, ECGs, cardiac MRIs, PULS tests and clean bills of health – the FAA will be putting many innocent airline passengers’ lives in harm’s way in the event a pilot loses control of his aircraft after suffering a major bloodclotting event (pulmonary embolism, stroke, etc.) or a myocarditis-related event, either of which can result in incapacitation, cardiac arrest, and death.”
Many airlines carry additional crew on long-haul flights to satisfy inflight rest requirements. One of these pilots could fill in during a medical event in one of the other pilots. However, on short-haul flights, no additional crew members are required. Consequently, a medical event in one pilot would result in the remaining pilot having to accomplish all the duties of the two-person crew all alone, adding considerably to the stress level. Consider the situation as your captain suffering the cardiac event, with a junior first officer now suddenly thrust into the high-workload situation of recovering the aircraft and passengers safely. Then imagine that same cardiac event happening suddenly at low altitude in an already high-workload task such as takeoff or landing. And then throw in bad weather. Such a scenario could very easily be unrecoverable and could result in the deaths of hundreds of people.
The letter goes on to highlight this circumstance:
“… a seizure that creates massive muscle stiffening and jerking of large muscle groups could be catastrophic if the pilot were on approach for landing, and actively flying the plane only a few hundred feet above the runway. A vaccinated pilot who suffers such a full-blown tonic-clonic seizure while on approach – such that the pilot could not maintain level control of the plane a few hundred feet above the tarmac, and uncontrollably and inadvertently dipped a wing thus causing the plane to cartwheel down the runway at landing – would likely cause not just massive injury and death to innocent passengers, but also create shocking monetary liability for the airline company and insurance carriers, potentially extending into the hundreds of millions USD.”
Here is where my own personal experience—similar to that of thousands of other government employees—becomes relevant. On 9 Sep 2021, President Joe Biden signed into effect Executive Order 14043 which required the covid vaccine for selected federal workers and others. I’d already done all my personal research, and even that body of knowledge available as early as the summer of ’21 was filled with reports of severe adverse effects and even deaths caused by the covid shot. It was easily clear to me that these shots were far from safe and effective despite what mainstream news outlets and the government hammered at us.
Shortly after the executive order was published, I and my FAA co-workers were required to upload into a database our vaccine status. I and many others declined. We then learned that exemptions would be allowed, and we were told to advise our immediate supervisors of our intent to file such an exemption request. I notified my supervisor as instructed. Shortly after that—all this activity was happening in a short period of time in the fall of 2021—I was advised that something called a “Disciplinary Period” had just been established. This Disciplinary Period, we were told, was to be a series of training events with FAA Human Resources, with the intent to coerce those of us who did not plan to get the shot to change our minds or else face disciplinary action, up to and including firing.
The government then really turned up the heat. I received two separate phone calls, one from my supervisor and the other from my Union Representative. In both calls, I was advised that if I retired to avoid the disciplinary period, that an unspecified amount of my retirement annuity could be confiscated. And just like that, there it was—the Jab or Job threat. Having enough of this coercion, I prepared and submitted a retirement package and was out of the FAA four days later. I was advised that I had missed entering the disciplinary period by just two days. Apparently, decades of flight test experience, thousands of hours of flight time in over 120 separate aircraft types, ten different type ratings, and millions of dollars invested in my training over the years were meaningless to the administration.
Perhaps you’re someone who doesn’t fly often, or even at all. You think you don’t have a dog in this fight. You would be wrong. Imagine the pilot of the aircraft flying overhead just after takeoff from your nearby airport suffering a fatal myocarditis incident, and she slumps over the controls. Unlike the circumstance of the recent Envoy Airlines incident where the other crew member—a highly experienced line check airman giving training that day to the captain under training—was able to recover the aircraft and bring it back to a safe landing, the other pilot in the aircraft over your head today was not able to do so and the plane crashed into your neighborhood. We are all at risk. Our country is on the wrong vector. The cockpit of the plane of state—shall we say—is unoccupied.
Part 3 - The Cover-Up
So what do we do now? We’ve learned that our nation’s pilots, flight attendants, air traffic controllers, and other aviation professionals were forced to take the Covid 19 shots by their companies or by the federal government or else lose their jobs through forced retirement or even outright firing.
We then learned of the emerging consequences of those mandates. Aviation professionals—among millions of other people in the world—are suffering severe cardiac events and even death because of these shots. The emphasis of this article is the increasing frequency of these events happening specifically to pilots. The effect of a major cardiac event happening to your pilot in a critical phase of flight such as takeoff or landing—high-workload events close to the ground—can be catastrophic to you as a passenger or even to you as an innocent person on the ground under the aircraft’s flight path.
Because of the vast number of pilots failing flight physicals, going on long-term disability, or even reporting for work unfit to fly since the rollout of the shot, it became apparent to the FAA medical community that a new problem had appeared. In such a case, examination of the extreme can be valuable for analysis. For example, given the increasing rate of these medical events in the pilot force, the logical extreme is that eventually there would not be enough pilots left to operate the nation’s airlines. By extension, all commerce provided by air would cease, and with that the country could come to a slow, grinding halt.
To give you an idea of the extent of this problem, recall how excited the government and the airlines were to announce that 95%...no!...98% of our pilots are vaccinated? Estimates are that 80% of the commercial pilots in the U.S. have taken the shot. According to Federal Aviation Administration data from 2022, there are just over 104,000 commercial pilots in America. Without treatment (emphasis mine), a mortality rate of approximately 20% in two years is expected in this group (editor’s note: this is the 5 year rate mortality rate after an initial case of myocarditis- this rate is reported in previous peer reviewed studies). The expected mortality rate in five years is much higher. Public math reveals that without treatment, we could lose over 20,000 pilots. Have you been paying attention to the hundreds of articles over the last few months related to the “Died Suddenly” phenomena? Based on what you should’ve been reading, does this number not seem totally plausible?
The aviation industry contributes extensively to the world’s economy. Should the aviation industry falter, then commerce, tourism, humanitarian aid, and even the job market would suffer. Trillions of dollars of goods are transported by air annually, with a huge percentage of e-commerce traffic delivered by air. Clearly the impact of the U.S. losing a significant number of our pilot force over the next several years would be catastrophic. Experienced, safe airline pilots are hard to replace
The FAA sees this; consequently, you need to know about a new development regarding the FAA’s flight medical exam requirements. The requirement for the heart exam portion of the flight physical regarding the allowable length of a parameter called the PR Interval (the start of the P-wave to the onset of the QRS complex) to be between 120ms to 200ms has been in effect for decades. Now, however, the FAA has lengthened this allowed PR Interval to 300ms and beyond. This is a huge change for this parameter!
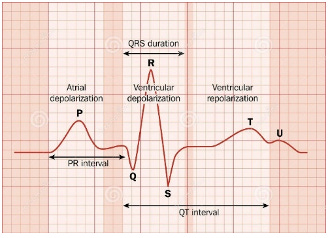
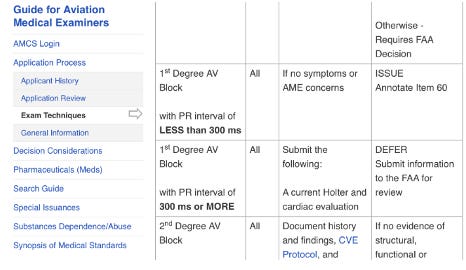
This much longer allowable PR interval—just published in October of 2022 per the FAA website’s guidance for aviation medical examiners—can mask major heart issues. (See in the figure the bold print that extends the PR Interval to 300ms and beyond.) This wording first appeared in October of 2022 and has been continued as recently as the 25 Jan 2023 revision. This change was done completely outside the required vetting procedure provided by the Notice of Proposed Rule making (NPRM) process. Such a major change, with such potentially lethal, catastrophic consequences to both aircrew and civilians is arguably criminal.
Until so many pilots began manifesting heart problems after receiving the Covid 19 shot, this had never been an issue. But with so many flight crews going on long-term disability, failing flight physicals, and other issues, the FAA lengthened the interval. But now, effectively, a vaxx-injured pilot could pass a flight physical, suffer a fatal cardiac event the next day, and be completely legal to do so. Said another way, a pilot could pass the flight physical with a major—even subclinical—heart issue just waiting to manifest. The very shot the government and the airlines mandated has caused the government to attempt to hide the problem it caused. The rub? The FAA refuses to acknowledge vaccine injuries in pilots, and also refuses to acknowledge any impact of pilot incapacitation because of vaccine injury on flight operations. Cover-up, indeed.
Epilogue
The good news is that once a problem is identified in a pilot, that person now has options. The goal of organizations such as US Freedom Flyers (US Freedom Flyers – We Stand For Medical Freedom!) and various medical professionals is to get these people the help they need to return safely to flight status.

Note, too, that the Freedom Flyers have litigation in progress against the FAA to right this wrong. If you want to donate to the litigation fund, please see the GiveSendGo campaign at and help the cause.
Below is a short list of different protocols in use and under development.
I-Recover – See the I-Recover Post-Vaccine Treatment page at
to view a comprehensive list of treatments for Post-Covid-Vaccine Syndrome. This document also provides an extensive discussion on definitions and pathologies of vaccine injuries.
A product called Cardio Miracle (cardiomiracle.com – no affiliation with the author) and other supplements like it that are based on nitric oxide help with clotting issues, since nitric oxide is essential for blood vessel flexibility, increased blood flow, and strengthened immunity.
Enhanced External Counter Pulsation (EECP) – This therapy uses large cuffs on your upper and lower legs. The cuffs fill with air, causing them to squeeze your legs. The cuffs on your lower legs squeeze first, then your upper leg cuffs squeeze next. The cuffs will then release the air. A computer times the squeezes so that they happen when your heart beats. With each squeeze, blood is forced back up to your heart. There are numerous articles on EECP available for your personal research.
If you’re reading this article and you’re an affected pilot or know someone who is—or you know anyone who might benefit from such treatments—please contact a trusted healthcare provider to investigate what might work for you or someone you know. If we as flight crew and passengers can get the word out to the rest of the flying public, we can be effective to help restore the level of safety of the National Airspace System to which we have been accustomed for decades. If nothing changes, it is just a matter of time until we suffer a major disaster. However, once the problem is actually acknowledged by a large enough percentage of the public and corrective action begins, together we can get our National Airspace System back on the right vector.
Flight Director for Apollo 13, Gene Krantz, and the exceptional team of hundreds of people at Mission Control as well as the courageous crew were able to get three astronauts safely back to earth. Everyone acknowledged the problem and worked together to achieve the goal. Now, however, we are witnessing a cover-up of vast proportions and implications. The government and the airlines are actually the cause of this ticking time-bomb. America, we truly do have a problem, and we must fix it.
I read this on Dr. Kevin Stillwagon's substack a few minutes ago. For a variety of reasons, I decided during the last few years that I do not want to fly again. We have been frequent flyers for the last twenty years, most often out of the country on mission trips. After the disastrous withdrawal from Afghanistan, I no longer felt my American embassy would have my back if I needed help. Things could change in an instant and I might be required to be jabbed to return home. The issue with injured pilots was the final straw. There's no reason for me to believe that the FAA or any other government agency cares at all about our safety.
Dr Malone, thank you for giving a platform to people like Brett Vance whose voices need to be heard. In his excellent interview with Tucker Carlson, Ed Dowd mentions that it was your support that multiplied his audience and enabled him to communicate a very important angle he has been researching on the covid scandal (health insurance trends among other things). I highly recommend Ed's conversation with Tucker, he is an inspiring and fascinating man (on Rumble in full)!
https://rumble.com/v2ailv0-tucker-carlson-interview-ed-dowd.html?utm_source=substack&utm_medium=email