
COVID Vax worsens long COVID--only 2% improved, 33% worse off
Deterioration was associated with Moderna (mRNA-1273) and persistent cough at vaccination


Yes, I accepted two doses of Moderna COVID vaccine. Again and again, I have been attacked for having done so by a wide range of haters. And as I have repeatedly explained, I did so for three reasons.
I was infected with the original SARS-CoV-2 strain (Wuhan 1) while attending an MIT computational drug discovery meeting in Boston at the end of February, 2020. I thought I was going to die, and so started taking various over the counter drugs that the team I was working with had identified as potential treatments for COVID based on computational docking modeling. The repurposed drug that really seemed to work for me was famotidine. Few are aware that this early peer-reviewed paper was the product of the subsequent research. But despite the beneficial effects I experienced from high-dose famotidine, I developed long COVID at a time when many disputed that this syndrome existed. As more and more began reporting that they were experiencing this syndrome, a new promoted narrative emerged: Accepting the mRNA vaccines would increase a suboptimal post-infection immune response and thereby overcome the symptoms of long COVID. So, that was reason #1 leading me to consider accepting the mRNA product.
Reason #2. I knew that I would need to travel internationally for various upcoming conferences being held in France and Italy. It was impossible to travel internationally without having documentation of receipt of one of these vaccines; the adenovirus-based gene therapy products (Janssen, AstraZeneca) were more toxic than the mRNA products, and the caterpillar cell-based protein vaccine was not yet available.
Reason #3. I called up an old colleague at the University of British Columbia, Dr. Pieter Cullis - he was the lead scientist/academic who developed the enabling lipid nanoplex formulations used by both Moderna and BioNTech. If anyone deserved a Nobel Prize for enabling these COVID gene therapy vaccines, it would be Pieter. In any case, I called him up and asked about what he and his team had done. He assured me that the toxicity and tissue-specificity issues I had encountered years before had been resolved with the formulations developed in his lab. I respected and believed him.
So, for these three reasons, I accepted the only “vaccine” product available in my part of Virginia (administered in a program run by the National Guard), which was the Moderna product.
My long COVID did not resolve, and if anything, it got worse. Furthermore, I developed life-threatening complications, none of which were known or acknowledged at the time. Most significant was hypertension with systolic pressure spiking above 220 mmHg together with tachycardia. Also, POTS, restless leg syndrome, tinnitus, and various other problems. My chronic long-COVID cough got worse. High probability I had developed myocarditis, although this complication was unknown/unreported at the time, and so I was not worked up for that.
With that background in mind, you can appreciate why this pre-print caught my eye.
This multicenter cohort study conducted across 33 emergency departments in five Canadian provinces examined factors linked to the deterioration of post-COVID-19 condition (PCC) symptoms in 476 patients who met the World Health Organization’s PCC criteria and received at least one SARS-CoV-2 vaccine dose 90 or more days after their initial infection.
Participants aged 18 and older were recruited between October 2020 and February 2022, and data were collected via telephone questionnaires assessing symptoms, vaccination status, and sociodemographic details; logistic regression models were used to identify associations. Results showed that 28.8% of participants reported worsening of symptoms following vaccination, while 71.2% experienced improvement or no change. Independent factors associated with deterioration included receiving the Moderna (mRNA-1273) vaccine (adjusted odds ratio [aOR] 1.81, 95% CI 1.15-2.84) and having a persistent cough at the time of vaccination (aOR 1.87, 95% CI 1.06-3.26), with no significant links to age, sex, or other sociodemographic variables.
The study suggests that potential immunoinflammatory mechanisms, such as heightened immune response or renin-angiotensin system dysregulation, may contribute to these outcomes, though limitations include self-reported data, modest effect sizes, and a lack of formal psychometric validation for the questionnaire. While affirming the overall benefits of vaccination, the findings advocate for further research into underlying pathways and personalized vaccination approaches for PCC patients, particularly those with persistent cough.
Mechanisms of PCC symptom deterioration
The deterioration of post-COVID-19 condition (PCC) symptoms following SARS-CoV-2 vaccination, as observed in some patients, may involve several interconnected immuno-inflammatory mechanisms. In a recent multicenter cohort study, approximately 28.8% of PCC patients reported symptom worsening after receiving a vaccine dose at least 90 days post-infection, with persistent cough at vaccination and use of the Moderna (mRNA-1273) vaccine identified as key risk factors (reference). A persistent cough in PCC often signals ongoing airway inflammation, bronchial hyperreactivity, residual mucosal damage, or vagus nerve involvement from a prior viral infection, potentially exacerbated by vaccination-induced immune stimulation (reference). This could indicate an active immune process in the lungs, where mRNA vaccines trigger a heightened response, amplifying systemic symptoms (reference). Dysregulation of the renin-angiotensin system (RAS) plays a central role: SARS-CoV-2 infection reduces angiotensin-converting enzyme 2 (ACE2) expression, leading to elevated angiotensin II levels that promote inflammation and sensory nerve sensitization in the airways, contributing to chronic cough and broader PCC flares (reference). Vaccination, particularly with mRNA formulations encoding the spike protein, may further disrupt ACE2 availability, though this remains debated, as some evidence suggests vaccines cause only transient, milder effects compared to infection (reference). The higher mRNA dose in Moderna vaccines elicits stronger humoral and cellular immunity, potentially worsening inflammation in susceptible individuals with pre-existing immune dysregulation or autoimmune tendencies (reference). Additional pathways include persistent spike protein presence post-vaccination, which can interact with ACE2 receptors or mannan-binding lectin, fostering autoimmunity, endothelial damage, hypercoagulation, and tissue hypoxia—mechanisms overlapping with long COVID itself (reference). Complement system dysregulation induced by microthrombi in acute COVID-19 may also be amplified, leading to excessive antibody responses correlated with deterioration (reference). Neuroinflammatory processes could explain associated cognitive symptoms, such as concentration difficulties, driven by similar immune dysfunction (reference). While vaccination’s overall benefits outweigh risks for most, these findings underscore the need for personalized strategies in PCC patients, especially those with inflammatory markers like persistent cough, and highlight shared pathophysiological traits between post-infection and post-vaccination syndromes (reference).
Trial Site News has published a brief review and analysis of the manuscript, which is republished below with permission from the publisher. Looks to me like yet another promoted pro-vax COVID narrative has failed the test of time and actual data. The results are entirely consistent with my personal experience.
Only 2% Improved, Nearly 1 in 3 Worsened: Canadian Study Upends Assumptions About Vaccination and Long COVID
For people already living with long COVID, this study suggests vaccination is not a one-size-fits-all experience. In a large Canadian cohort, most participants reported no change in their post-COVID symptoms after vaccination, only about 2% reported clear improvement, and nearly one in three (29%) said their symptoms worsened. The risk of deterioration was higher among those who received the Moderna (mRNA-1273) vaccine and among patients who still had a persistent cough at the time of vaccination—signals that point toward underlying inflammation or immune activity as possible drivers. The implication is straightforward but important: post-infection vaccination may help a small minority, leave most people unchanged, and worsen symptoms in a substantial subset, challenging the blanket message that vaccination uniformly improves long COVID. While this preprint relies on self-reported outcomes and should not change care overnight, it raises a credible caution flag and underscores the need for more individualized guidance, better informed consent, and careful clinician–patient conversations as policies evolve for people already struggling with post-COVID illness.
Study Summary
Led by Malika Seydou Beidari along with emergency medicine professor Patrick M. Archambault and investigators across the Canadian COVID-19 Emergency Department Rapid Response Network (CCEDRRN) (including Université Laval and partners), a preprint reports a multicenter Canadian cohort study asking a pointed question: among adults who already met the WHO definition of post-COVID-19 condition (PCC) or long COVID, what factors predict symptom deterioration after a SARS-CoV-2 vaccine dose given ≥90 days post-infection? In 476 PCC patients followed by telephone questionnaires, 28.8% (137/476; 95% CI 24.7–32.9%) reported worsened PCC symptoms after vaccination, while 71.2% reported no change or improvement. In adjusted models, deterioration was associated with Moderna (mRNA-1273) (aOR 1.81; 95% CI 1.15–2.84) and persistent cough at vaccination (aOR 1.87; 95% CI 1.06–3.26). If confirmed, this challenges the simplified public narrative that vaccination uniformly improves established long COVID—suggesting heterogeneous, patient-profile-dependent responses.

Study Design
This multicenter observational cohort drew from 33 emergency departments across five provinces, enrolling adults who tested SARS-CoV-2 positive (Oct 2020–Feb 2022), then completed PCC symptom surveys at 6 and/or 12 months (Nov 2021–July 2022). PCC was defined using the WHO criteria, and the “reference dose” was the first vaccine dose ≥90 days after ED index infection. Outcome was self-reported symptom change after vaccination, analyzed with multivariable logistic regression.
Findings
A larger share of those receiving Moderna ≥90 days post-infection reported deterioration (38.9%) versus pooled comparators (~25.5% for AstraZeneca+Pfizer combined, per appendix). Sociodemographics (age, sex) were not associated with deterioration. Notably, the “risk signal” clustered around an inflammatory respiratory phenotype (persistent cough), aligning with hypotheses about immune activation in some PCC subgroups.
Red Flags & Limitations (ESI 2.0 Lens)
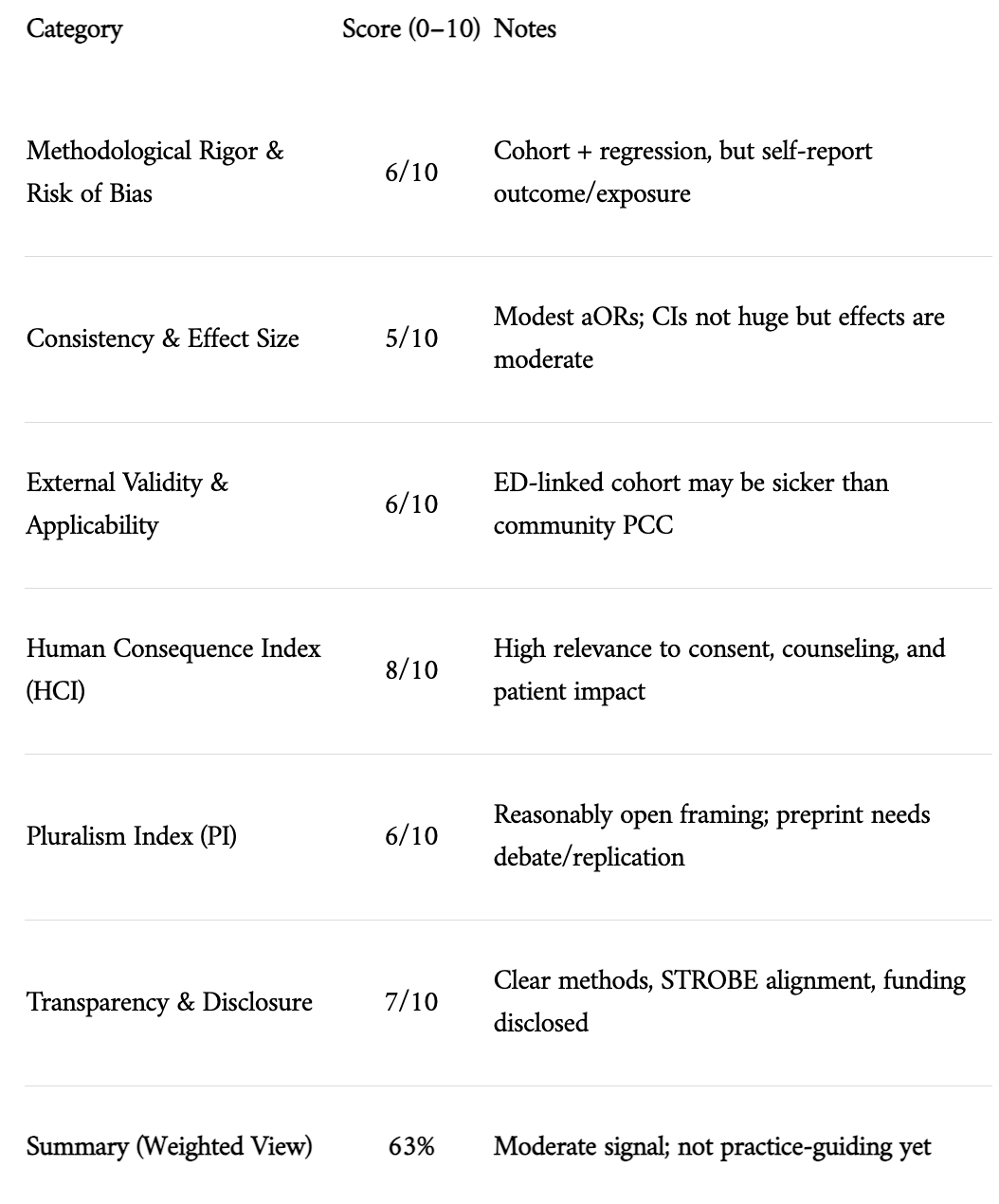
Limitations included self-reported vaccination and outcomes, lack of objective biomarkers, and unknown duration of post-vaccination worsening (transient vs persistent). Pooling “no change” with “improvement” can mask nuance. HCI: the findings matter because they touch autonomy and informed consent for people living with PCC. PI: the work is transparent about uncertainty, but as a preprint, it needs independent replication and fuller mechanistic exploration.
Conclusion & Implications
This preprint offers a consequential signal: about 3 in 10 PCC patients reported worsening after post-infection vaccination, with higher odds in Moderna recipients and those with persistent cough. In summary, this study provides moderate-strength evidence of risk heterogeneity in established PCC and underscores the need for stratified vaccination guidance and mechanistic studies in long COVID populations.
TrialSite Evidence Strength Indicator™ (ESI 2.0)
The people who generated the pretext and forced the "solutions" on the world; it is they who owe explanations. And none will suffice.
The hunch, or gut feeling, might be counted as irrelevant in the circles of science/research. I remember no single cue prompting my decisions. I do remember barrages of infomercials and voice recordings played overhead at a Kroger or a CVS. Ad spots, with effeminate males literally bounding out of bed, singing that today was their day to get the "vaccine." That feeling that something was terribly, terribly wrong was creeping into my thoughts.
I guess we are going to study this to death until 2030 when EAU expires. In the meantime we will continue to reprogram the ribosome machinery inside the human cell and change the proteins that the cell is supposed to be producing to keep the body healthy. The mRNA is just interfering with normal cellular process in uncontrollable ways and we continue to go down this path. Why?