
DEI/Woke Medicine Forever
Emory Medical School OB/GYN Professor Nisha Verma demonstrates how American medicine has been transformed


During recent testimony, both Senator Josh Hawley and the rest of the world were provided a lesson in the distortion of the modern US medical system that has occurred under the influence of cultural Marxism, DEI programs, and woke ideology. Under questioning, Emory Professor Dr. Nisha Verma could not or would not answer Hawley’s straightforward question to this Board Certified Obstetrician/Gynecologist, “Can Men Get Pregnant?” For the majority of those paying attention throughout the English-speaking world, the resulting exchange was bizarre. What most do not appreciate is that the inability of a highly credentialed Obstetrician/Gynecologist to answer this straightforward, biologically obvious question is both a symptom of the present state of medical education and a predictor of the future of American Medicine.
With her condescending testimony, Dr. Nisha Verma has provided all who care to watch and think with a perfect example of the consequences of decades of higher educational DEI policies and cultural Marxist ideology. Her careful use of politically acceptable terminology to side-step acknowledging a straightforward, fundamental biological truth is the product of decades of successful training and struggle sessions that now enable her to survive and thrive in an academic medical culture driven mad by infiltration and domination by cultural Marxists.
Most are aware of the impact of the Diversity, Equity, and Inclusion (DEI) policies that have evolved, been propagated, and been enforced throughout the US government, industry, and academia over the past decades. Fewer are aware of the 2023 SFFA Supreme Court decision most associated with DEI debates — it prohibited race as a direct factor in college admissions and indirectly intensified challenges to DEI elsewhere, without eliminating it entirely. Properly designed programs (avoiding quotas, preferences, or stereotypes) continue to be defensible under existing law.
On January 20, 2025—his first day in office for his second term—President Donald Trump issued Executive Order 14151, titled “Ending Radical and Wasteful Government DEI Programs and Preferencing.” This order directed federal agencies to terminate all diversity, equity, and inclusion (DEI) and diversity, equity, inclusion, and accessibility (DEIA) mandates, policies, programs, preferences, and activities. It specifically required the elimination of DEI offices, positions (such as Chief Diversity Officers), equity action plans, equity-related grants or contracts, and DEI performance requirements for employees, contractors, or grantees. The order revoked prior Biden-era executive actions, including Executive Order 13985 (”Advancing Racial Equity and Support for Underserved Communities Through the Federal Government”), and aimed to end what it described as “illegal and immoral discrimination programs” in areas like federal hiring, military operations, and airline safety.
The following day, on January 21, 2025, Trump issued Executive Order 14173, titled “Ending Illegal Discrimination and Restoring Merit-Based Opportunity.” This order revoked longstanding affirmative action-related executive orders, including Executive Order 11246 (issued by President Lyndon B. Johnson in 1965, which required federal contractors to implement affirmative action programs to prevent discrimination). It mandated that federal agencies terminate all “discriminatory and illegal preferences, mandates, policies, programs, activities, guidance, regulations, enforcement actions, consent orders, and requirements.” For federal contractors and grant recipients (including American Medical Colleges, which are heavily subsidized by the federal government), it introduced new certification requirements: They must affirm compliance with federal anti-discrimination laws and certify they do not operate “illegal DEI programs,” with non-compliance potentially triggering liability under the False Claims Act. The order also directed agencies to prioritize enforcement against unlawful DEI practices in the private sector.
Additionally, on January 20, 2025, Trump issued a related Executive Order titled “Defending Women From Gender Ideology Extremism and Restoring Biological Truth to the Federal Government,” which intersected with DEI by establishing a federal policy recognizing only two biological sexes and terminating gender identity-related policies, programs, and protections in areas like federal employment, education, and sports.
As demonstrated by the testimony of Emory Professor Dr. Nisha Verma, these Executive Orders have been widely disregarded or otherwise side-stepped through application of creative language and logic. In the context of American Medicine, the systemic mechanisms by which compliance with these orders has been circumvented have been covered in the following essay, which documents the processes, bureaucratic tricks, and language used as well as the central control mechanisms employed by the medical guild known as the “Association of American Medical Colleges” (AAMC), which controls what American Medical schools must teach, how they are to teach it, what criteria they are to use in accepting medical students, and how they are to be tested upon graduation before they are allowed to practice medicine. Through affiliate relationships, the AAMC also influences the policies, culture, and practices of virtually every other specialty medical guild in the United States, as well as the various State medical boards that enforce what are considered acceptable medical practices and culture. And the AAMC bureaucracy is all in on DEI, cultural Marxism, and woke culture, despite what SCOTUS and POTUS have to say.
The truth is, even if she were not fully indoctrinated into gender-fluid logic and language, Emory Professor Dr. Nisha Verma could not survive and thrive in the current culture of American academic medicine without mastering the art of avoiding the straightforward question posed by Senator Hawley.
The Association of American Medical Colleges is the Medical Guild driving DEI and Censorship

The Association of American Medical Colleges (AAMC) is the Medical Guild driving DEI and Censorship in American Medicine
This exemplary parable kindly provided by Hawley and Verma illustrates four fundamentals of modern US medicine.
The first is that the logic and culture of DEI, cultural Marxism, and wokeism are firmly embedded throughout the entire academic enterprise, from kindergarten through professional education and beyond. Colleagues in the legal profession tell me that the same culture, trends, and enforcement mechanisms pervade the American Bar Association legal Guild.
The second is that the historic culture and practice norms of American Medicine are being rapidly replaced with each graduating class of medical students. Student admission is no longer driven primarily by merit; now it is a product of subjective cultural and diversity criteria, all justified as advancing inclusiveness objectives. One might imagine artificial intelligence as the eventual savior from medical care dominated by physicians selected for their ubiquitous obeisance to cultural Marxism and woke ideology, but the AAMC and its affiliate organizations are now establishing guidelines, norms, and enforcement policies on which AI future medical care providers are allowed to use.
The third is more subtle. Those perplexed by the question of how the now clearly seen (in hindsight) as bizarre, non-scientific, arbitrary, capricious, and counterproductive medical/public health advice and practices during COVID were propagated throughout the entire western medical system, in the parable of the Hawley and Verma testimony, we can see how this was accomplished. The modern medical corps has been selected, trained, and staffed for compliance and obedience to authority, not for independent thought. This is a central feature, not a bug.
And the fourth is even darker. For those who are not culturally aligned with woke ideology, the future of the Medical care that they are most likely to receive will be a bitter pill. They will have to learn to adapt to the language and logic of cultural Marxism and “utilitarian bioethics”, or they will be subjected to derision, ridicule, and struggle sessions until they do. Because the future of American Medicine and medical care is being mapped and developed by Emory Professor Dr. Nisha Verma and her cultural comrades.
The need to reject Utilitarian Bioethics and return to fundamentals
In its Code of Medical Ethics, the American Medical Association states that “Informed consent in medical treatment is fundamental in both ethics and law. Patients have the right to receive information and ask questions about recommended treatments so that they can make well-considered decisions about care. Successful communication in the patient-physician relationship fosters trust and supports shared decision making.”
In its Public Health Code of Ethics, the American Public Health Association asserts that “the effective and ethical practice of public health depends upon social and cultural conditions of respect for personal autonomy, self-determination, privacy, and the absence of domination in its many interpersonal and institutional forms.”
Utilitarian Bioethics, Medical Socialism and the State

“Leaders create culture. Culture drives behavior. Behavior produces results.”
How did this happen?
Step by step, in a ratcheting fashion, in the same way that all other totalitarian systems develop. In the current case, all justified by the best of intentions.
Diversity, Equity, and Inclusion (DEI) as a modern, unified framework and term emerged gradually in the late 20th and early 21st centuries, particularly in corporate, educational, and organizational settings. It evolved from earlier civil rights-era policies focused on combating discrimination and promoting equal opportunity.
The foundational concepts behind DEI trace directly to affirmative action policies in the United States, which aimed to proactively address historical discrimination and ensure fair treatment in employment, education, and contracting.
The term “affirmative action” was first introduced in federal policy by President John F. Kennedy in March 1961 via Executive Order 10925. This required government contractors to “take affirmative action” to ensure fair employment practices regardless of race, creed, color, or national origin. It marked the initial governmental promotion of proactive (rather than merely passive) non-discrimination measures to achieve equity.
President Lyndon B. Johnson significantly expanded and promoted these ideas. In September 1965, he issued Executive Order 11246, which strengthened requirements for federal contractors, added protections based on religion and (later) sex, and mandated affirmative action programs. Johnson famously articulated the need for such measures in his 1965 Howard University speech, arguing that equal opportunity alone was insufficient after centuries of discrimination — “You do not take a person who, for years, has been hobbled by chains... and then say, ‘You are free to compete with all the others.’”
These policies were part of the broader Civil Rights Movement, building on the Civil Rights Act of 1964 (signed by Johnson), which outlawed discrimination in employment and public accommodations. Early corporate implementations followed: For example, Xerox established one of the first Employee Resource Groups (ERGs) in 1965 (led by Black employees advocating for pay equity), and by the 1970s–1980s, companies began widespread diversity training in response to these federal mandates.
Emergence of the Modern “DEI” Framework and Term
The specific acronym DEI (Diversity, Equity, and Inclusion) gained prominence later:
In the 1980s–1990s, as affirmative action faced backlash (e.g., under Reagan), corporations reframed diversity efforts as a business advantage (e.g., improving innovation and performance), shifting from legal compliance to voluntary inclusion strategies. Consultants and academic scholars promoted this evolution.
The full DEI terminology became widespread in the 1990s–2000s in HR, corporate, and academic contexts, expanding beyond race/gender to include broader identities (e.g., disability, LGBTQ+, age).
Corporate DEI surged dramatically after events like the 2020 murder of George Floyd, leading to widespread commitments, dedicated teams, and billions in investments.
No single individual is credited as the sole “founder” of DEI. Historians describe it as an evolution driven by civil rights activists, policymakers (especially Kennedy and Johnson), corporate leaders, and later consultants/academics. Some sources credit figures like Lewis Brown Griggs (early 1980s) for popularizing “diversity and equity” language in training.
What can be done about it?
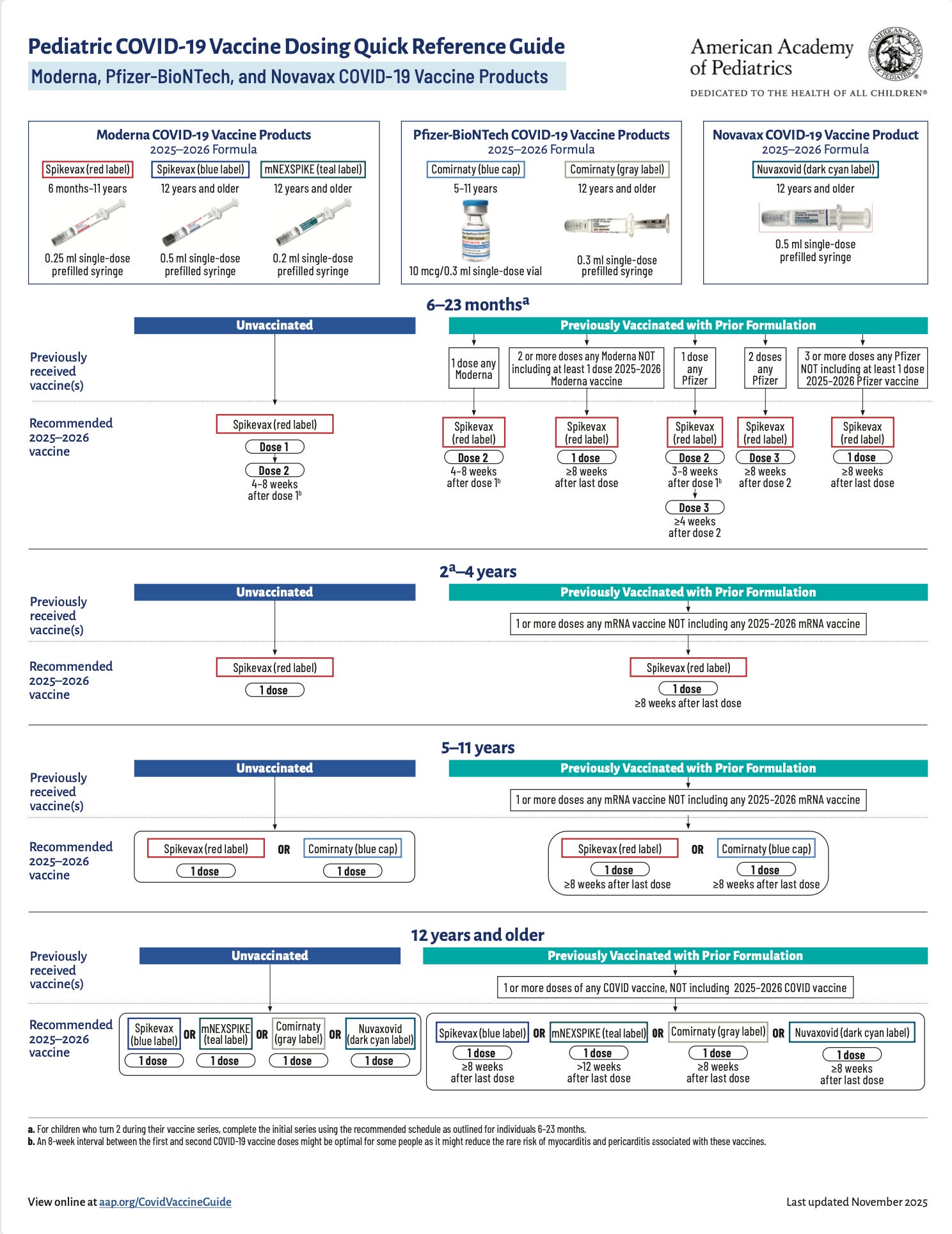
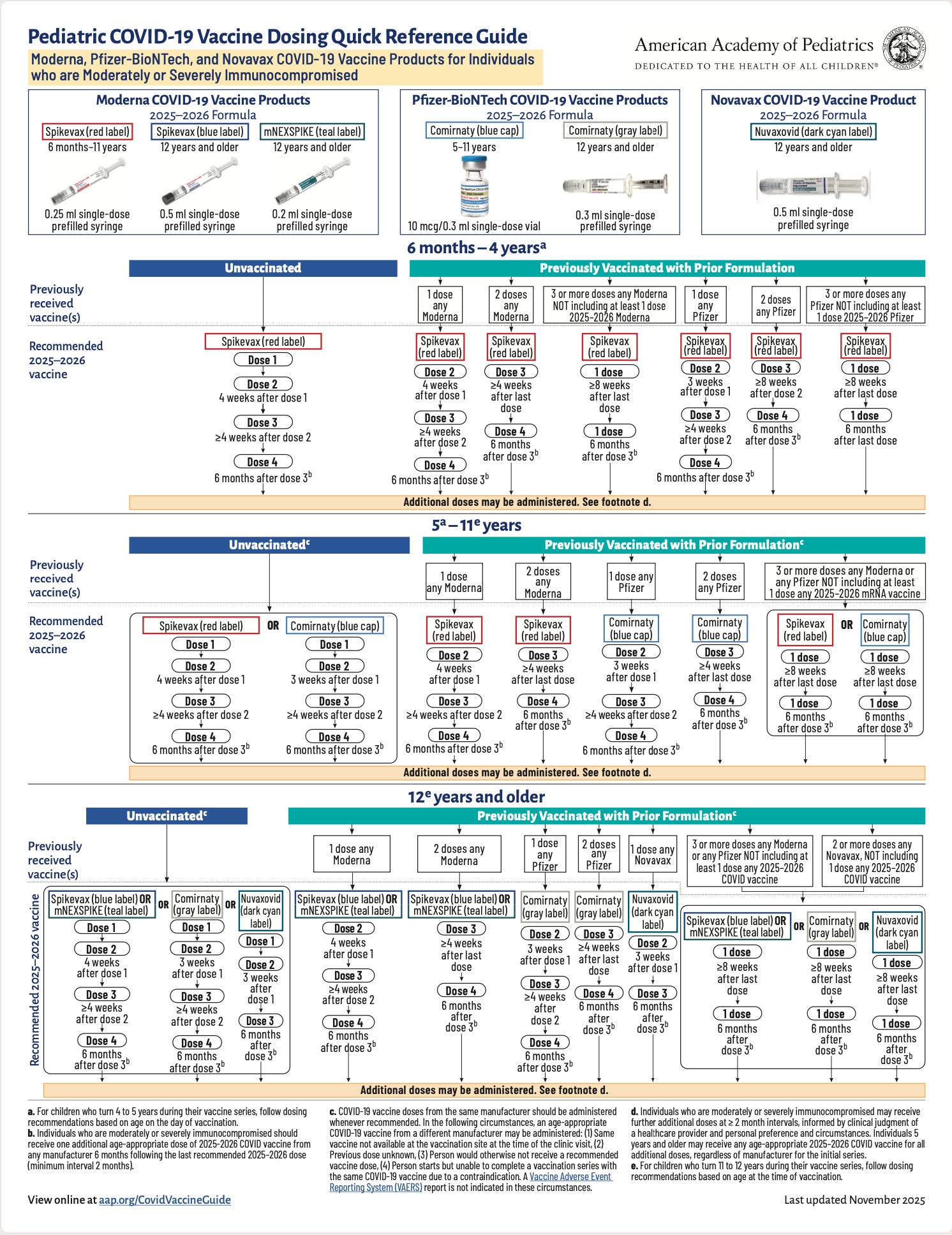
In terms of the broader issue of the various professional guilds that have now completely endorsed and absorbed DEI and cultural marxism, it may be necessary to apply legally acceptable processes to break up what is essentially monopolistic powers to regulate their respective industries and sectors. The Federal government has taken a lassez-faire approach to the professional guilds, preferring to allow them to self-regulate. As with any monopoly, this has resulted in reduced efficiency, corruption, barriers to innovation, higher prices for consumers, elitism, systematic censorship, and enforcement of accepted guild member norms and practices. The events of the COVID crisis were just one very obvious manifestation of these problems, which are likely to become increasingly dysfunctional. To provide one example, consider the new child and adolescent COVID vaccination guidance from the American Academy of Pediatrics medical guild.
On a more pragmatic level, individuals who are uncomfortable with the culture and practices of increasingly dominant “woke”, utilitarian, protocol-driven medical practitioners are going to have to more actively physician shop or just suck it up and deal with the new bosses and faces of American medicine. There are still some older physicians, often nearing retirement, who maintain private practice and have not yet come under the thumb of the dominant hospital/insurance/pharmaceutical/Obamacare axis. These are often private “family practice” offices or have migrated to various alternative approaches, such as “integrative” or “wholistic” medicine. One organization that has historically represented alternative and libertarian-leaning medical care providers is the Association of American Physicians and Surgeons (AAPS) - founded in 1943.
Wikipedia offers the following derisive assessment of AAPS, which for many may sound like an endorsement:
The Association of American Physicians and Surgeons (AAPS) is a politically conservative non-profit association that promotes conspiracy theories and medical misinformation, such as HIV/AIDS denialism, climate change denial, the abortion–breast cancer hypothesis, and vaccine and autism connections, through its official publication, the Journal of American Physicians and Surgeons, which masquerades as a legitimate scientific journal. The association was founded in 1943 to oppose a government attempt to nationalize health care. The group has included notable members, including American Republican politicians Ron Paul, Rand Paul and Tom Price.

For those who are uncomfortable with the corporatist medical sell outs and academic culture warriors, and who value medical care providers that actually respect the fundamentals of 20th century medical ethics, you may wish to look for AAPS members to provide your medical care.
In Conclusion
What does AAPS have to say about DEI in medicine?
1. Our country has been besieged by the Marxist-based ideology, known as “Diversity, Equity, and Inclusion,” which is infiltrating the practice of medicine through medical schools, biomedical research, hiring practices, and government regulations. Intrusion of DEI ideology into medical education and medical care is dangerous for patients and compels AAPS to issue this statement.
2. The ethical foundation of medical care dates back to the Oath of Hippocrates and obliges physicians to provide the best possible care individualized for each patient. Furthermore, safe, ethical, and high–quality care requires individuals who have the intellectual capacity, motivation, academic achievement, and moral compass to successfully negotiate medical school, training, and ultimately the responsibility of rendering care for their patients. DEI dogma promotes false ideology and mandates that are antithetical to these obligations and requirements.
3. Standards for students selected for medical school and postgraduate training, or for any physician, must be the same regardless of race, gender or other social metrics, and include a level of competence measured by academic achievement and standardized tests. Standards must not include adherence to, or promotion of, ideologies that contradict fundamental Hippocratic principles of medical ethics.
4. Patients must not be prioritized, or discriminated against, based on their race, gender or any other politically favored, or disfavored, status.
5. Our merit-based nation has been the most successful in history and has spent decades promoting equal opportunity for all citizens, celebrating achievement and supporting special needs. America has raised the standard of living for the greatest number of its people, while nations that embrace ideologies that disparage merit tend to decay into widespread poverty.
6. Vigorous and urgent actions must be launched to eliminate the destructive DEI ideology from every aspect of the medical profession before it is too late. Patients’ lives depend on it.
Speaking of woke, captured, and corrupted Medical Guilds, this provides a textbook example ….
American Academy of Pediatrics Pediatric COVID-19 Vaccine Dosing Quick Reference Guide
We, the American people, outnumber the AAMC. At 82, I no longer need an OB doctor. However, I have decided that my first question at every dr visit from now on will be: “Can a man give birth?” If I get an affirmative response, I will walk out saying, “I insist on a Dr who understands science.”
If thousands of us do that we can make a difference.
The last question Senator Hawley should have asked this woman is:
Given your inability to properly answer one of the most basic medical questions it is possible to ask, a question most second graders could answer easily, can you give this committee a good reason why we shouldn’t begin proceedings to have your medical credentials/licenses removed effective immediately?