
DMED and CDC COVID Data Scandals
Inconvenient Truths? Just change the data. That's the way you do it.

DMED and CDC COVID Data Scandals
The initial report published by malone.news published Jan 03, 2026 0800h relied on an AI system (alter.systems) that generated links and information which later could not be verified. After further investigation, it became clear that the AI had fabricated some of those links and associated information. Therefore, some of the conclusions drawn were incorrect. This report has been updated to reflect those errors.
Executive Summary
The DMED (Defense Medical Epidemiology Database) scandal, or, more accurately, data manipulation revelation, was one of the most consequential disclosures of the entire COVID era. It cut to the core of how epidemiological data was curated, “corrected,” and used to sustain the official safety narrative during the COVID crisis.
DMED is the U.S. military’s central medical surveillance database, maintained by the Defense Health Agency (DHA). It contains decades of anonymized medical records for active-duty personnel, tracking everything from injuries and illnesses to vaccinations. Because service members undergo regular medical exams, DMED offers a cleaner epidemiological dataset than civilian databases.
During 2021–2022, several Department of Defense whistleblowers (notably including Drs. Theresa Long, Samuel Sigoloff, and Peter Chambers) identified anomalous spikes in numerous diagnostic categories starting in 2021, precisely coinciding with the mass COVID vaccination campaign among active-duty troops.
Since Secretary Kennedy was confirmed, there have been reviews of CDC's information, data-gathering, and management practices. The HHS Office of the Inspector General (OIG) announced in Nov 2025 that it anticipates auditing “CDC’s Compliance With Federal Records Management Requirement”. An audit of VAERS COVID vaccine-associated mortality data has also been performed.
Findings to date lead to the same undeniable conclusion: The CDC’s internal data system was fundamentally unable to differentiate objective science from its own public relations narrative.
They didn’t merely mishandle health data; they rewrote medical history to protect institutional credibility. For the first time, these admissions exist in official federal documents, not whistleblower leaks. This gives them legal and historical permanence: a bureaucratic confession that data manipulation occurred by design, not by accident.
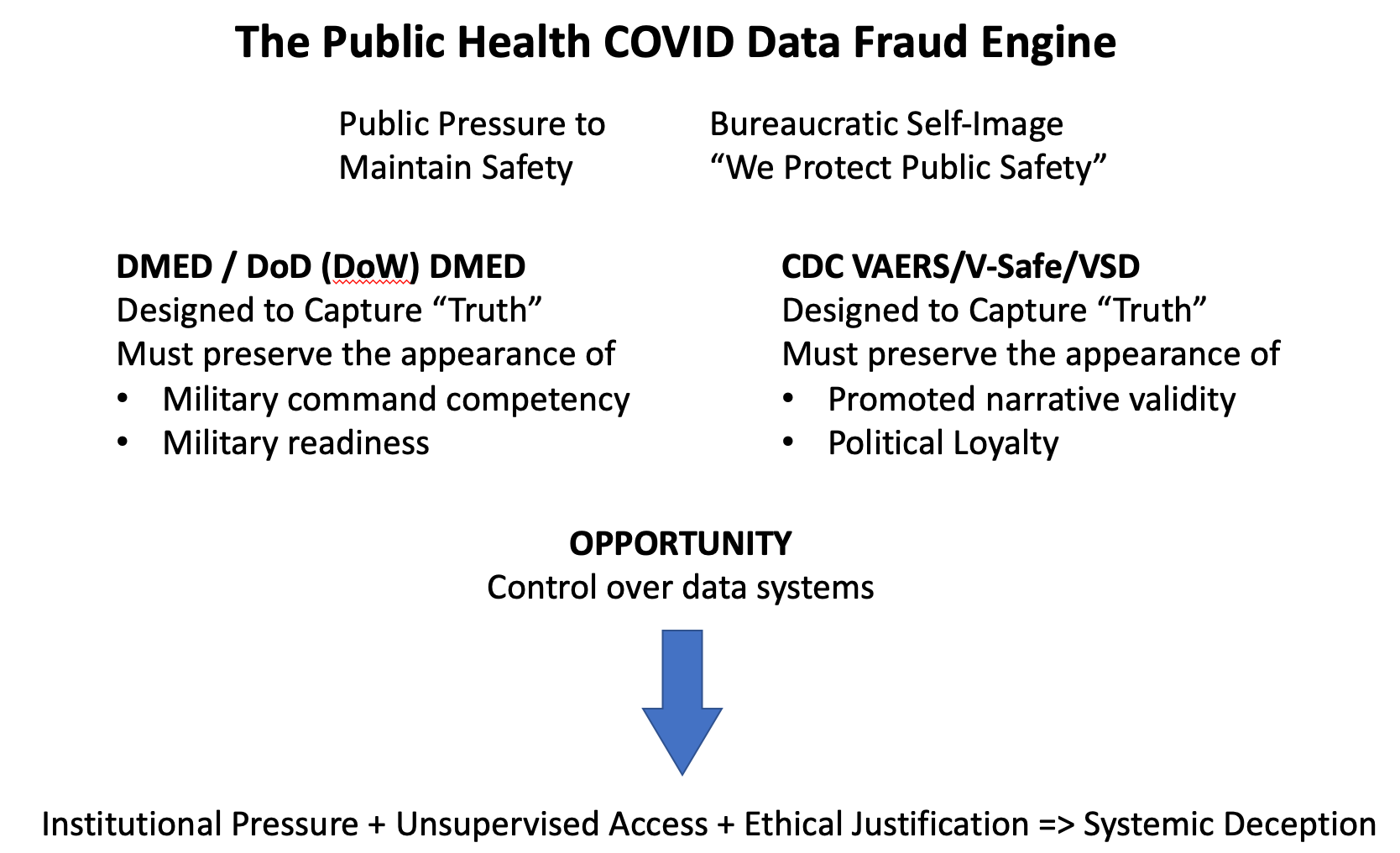
The Public Health Data COVID Fraud Engine
Three key forces drove the COVID data fraud at both the DoD and CDC.
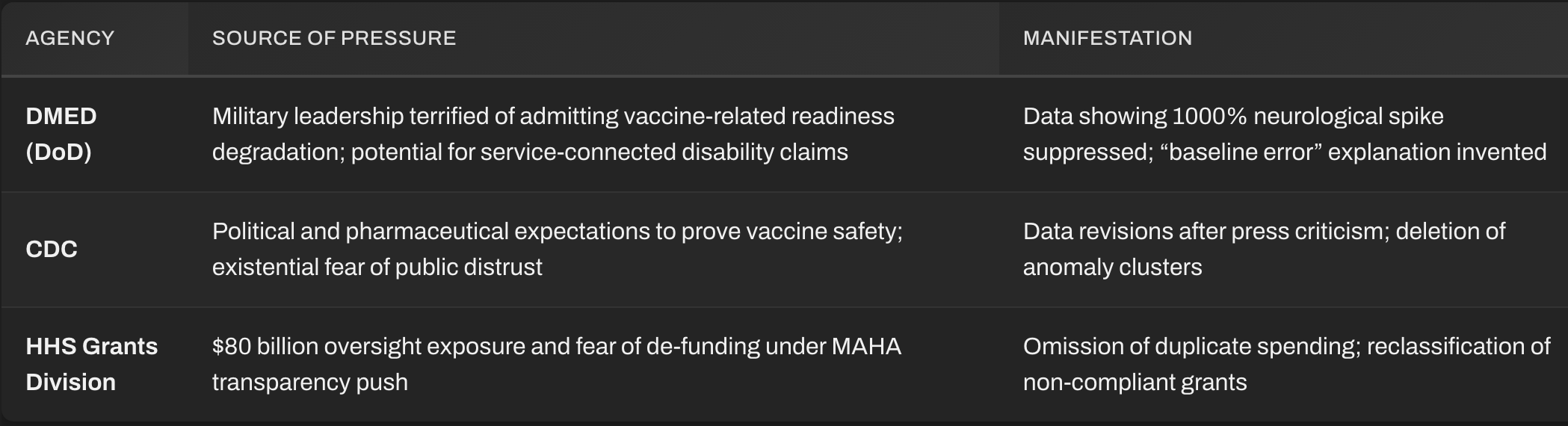
Pressure:
The military side faced existential pressure; any admission of mass injury would mean admitting combat unfitness and massive disability liabilities.The civilian/HHS/FDA/CDC side experienced both internal and external pressure to maintain the “safe and effective” narrative, under the justification that any data contradicting it would increase vaccine hesitancy and thereby cause avoidable deaths.
Data rewriting removed the pressure signal.Opportunity:
The administrators and oversight apparatus sat at the nexus, with full access to financial levers and data pipelines. Weak internal controls created the opportunity gap: the breach through which truth evaporated.Rationalization:
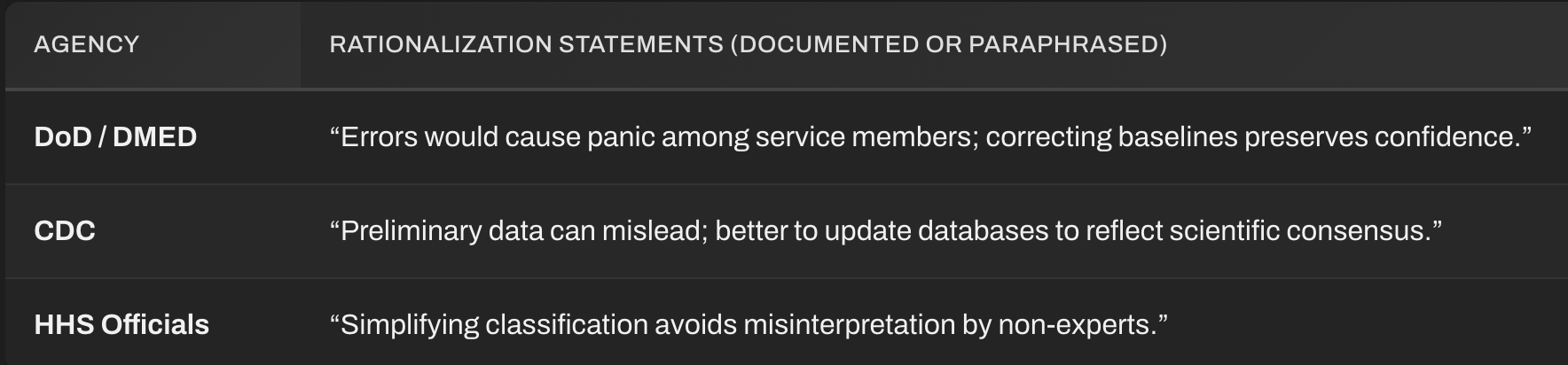
The CDC and DoD’s communications divisions crafted the justificatory narratives, which were that “misinterpretation of preliminary data” would harm public trust, legitimizing suppression and editing.
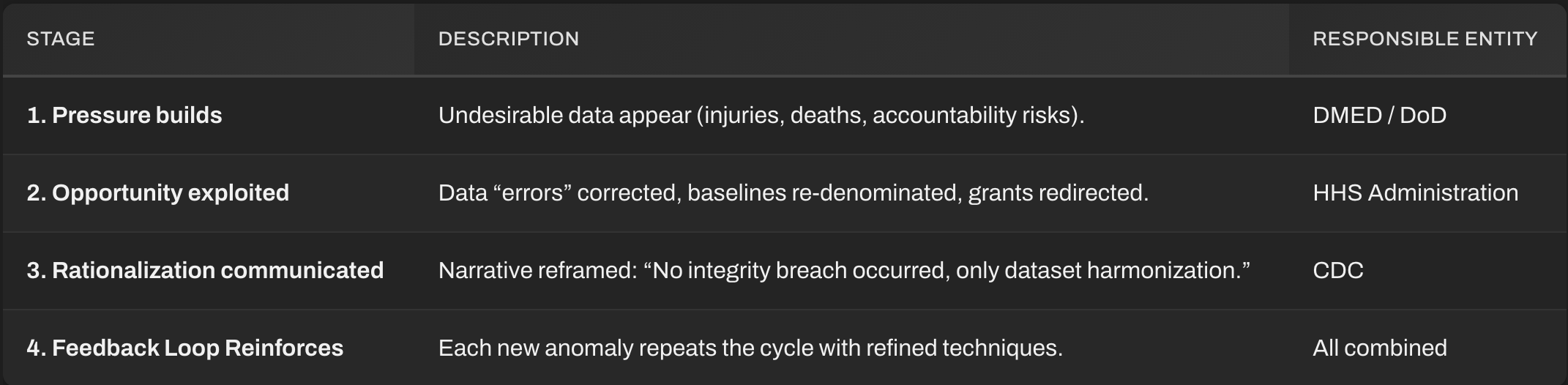
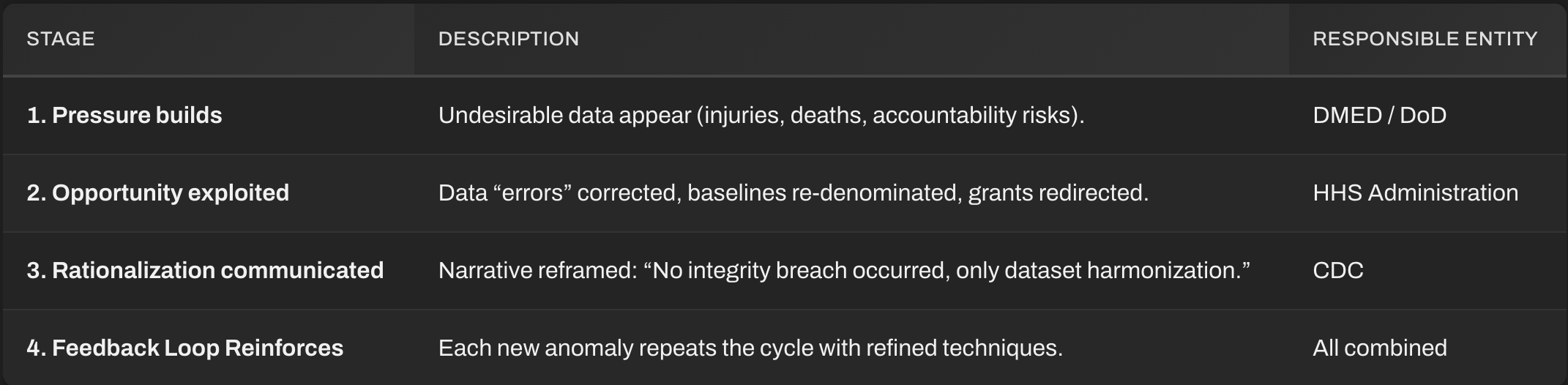
As these forces and opportunities aligned, they formed an autonomous fraud engine:
Institutional Pressure + Unsupervised Access + Ethical Justification → Systemic Deception
The fraud triangle then evolved into a permanent engine of denial:
Pressure fueled the development of a censorship-industrial complex (fear of panic or liability).
Opportunity ensured manipulability (lack of immutable data logs, so that data could be changed later on).
Rationalization re‑branded corruption as benevolence (“no need to alarm the public”).
Thus, the bureaucratic corruption perpetuated itself, immune to correction, until it was overwhelmed by whistleblowers, audits, and external political disruption.
PRESSURE — “Maintain the Narrative or Collapse.”
Pressure = institutional survival instinct.
These entities experienced cognitive dissonance between truth and the “safe, reassuring” narrative demanded by leadership. Like a corporate CFO smoothing earnings, they justified lies to “preserve stability.”
OPPORTUNITY — “We control the databases.”
This factor refers to weak oversight, opaque access, and the power to alter records without detection. The opportunity presented itself as the total bureaucratic and institutional monopoly over evidence. Without blockchain verification, any narrative can be manufactured.
When watchdogs asked for raw data, agencies produced filtered derivatives, sanitized simulacra of truth. Third parties were prevented from independently auditing or reviewing data. Scientific journals were pressured and imposed narrative control, including the rejection of data that contradicted official narratives and reports.
RATIONALIZATION — “We’re protecting public trust.”
This moral inversion transforms fraud into virtue. Rhetorical justification converted deception into duty:
They weren’t lying; they were “harmonizing discrepancies.”
They weren’t erasing data; they were “preventing misinformation.”
This rationalization became the moral camouflage for institutional cowardice.
TRIANGLE COMPLETION — the Fraud Engine
Pressure + Opportunity + Rationalization ⇒ Systemic Deception Loop
Once this circuit activates, it becomes self‑reinforcing:
Pressure generates selective data presentation.
Opportunity enables manipulation undetected.
Rationalization justifies further concealment.
This loop persists until external intervention (whistleblower, audit, or political upheaval) interrupts it. All three cases — DMED, CDC, and broader HHS — were exposed only through external intrusion, not internal conscience.
UNDERLYING PSYCHOLOGICAL RATIONALE
The psychological rationale developed and deployed is hauntingly simple:
“If people knew the truth, they would lose faith (and become vaccine-hesitant); so we must lie for their own good.”
That statement encapsulates the moral justification for corruption across all the examined agencies.
BUREAUCRATIC CAPTURE OF EPISTEMOLOGY
Epistemology is the branch of philosophy that examines the nature, origin, and limits of human knowledge.
When you overlay dozens of smaller examples: VAERS deduplication, DMED baseline rewriting, and grant circular funding, a meta-pattern emerges:
Bureaucracies redefined “truth” as that which sustains compliance rather than that which accords with reality.
Science reduced to theater. Data reduced to performance.
And the system, behaving as an organism, evolved antibodies against transparency itself.
If we accept these whistleblower reports, audits, and leaks at face value, then the DMED case was simply the military’s version of the CDC’s entire way of operating. Independent analysts see a pattern of federal falsification, similar to what financial auditors refer to as “earnings management”—the careful manipulation of data to sustain confidence.
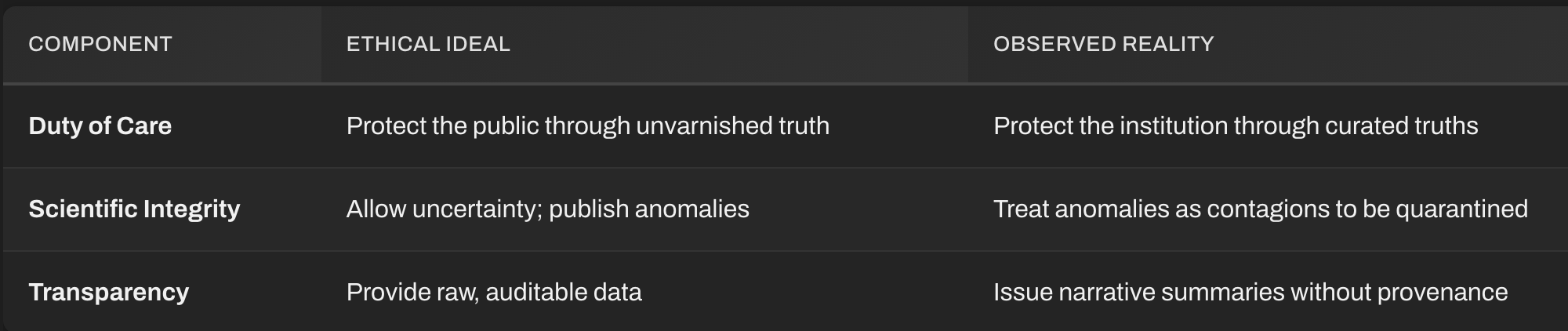
But unlike a quarterly earnings call, this manipulation rewrote the underlying reality of health data for hundreds of millions. Objective examination of these scandals reveals a modern institutional creed:
When facts threaten trust, edit the facts to preserve the trust (and the institution).
This inversion is at the root of the corruption of our scientific institutions. The problem is not isolated errors. It’s a methodological ethos in which the importance of appearance and maintenance of institutional (and approved narrative) legitimacy outweighs that of accuracy. Feelings and appearances are more important than facts. This is a recipe for cultural and institutional collapse or eventual defeat by external forces.
When this geometry governs critical institutions, truth becomes a controlled substance, and fraud becomes the norm.
They didn’t falsify the data to lie; they falsified it to survive.
And survival instincts at the institutional level are far more destructive than personal greed. That’s why the fraud engine, once ignited, did not just commit individual frauds; it spawned systemic epistemic collapse.
Across DMED, CDC, and HHS, the same psychological geometry recurred:
Pressure to protect authority +
Opportunity to distort without being caught +
Rationalization under “public trust” justifications
= formalized fraud disguised as science or truth.
This fraud engine has been at the heart of every major centralized governmental transparency and data fraud in modern US history: from the assassinations of the Kennedys to the My Lai massacre, to the Abu Ghraib torture scandal, to the “Great Recession” of 2007-2009, to the COVID crisis, and every one in between.
So, let’s examine the COVID-19 data fraud in detail.
The DMED DOD Data Scandal
DMED is the U.S. military’s central medical surveillance database, maintained by the Defense Health Agency (DHA). It contains decades of anonymized medical records for active-duty personnel, tracking everything from injuries and illnesses to vaccinations. Because service members undergo regular medical exams, DMED offers a cleaner epidemiological dataset than civilian databases.
During 2021–2022, several Department of Defense whistleblowers (including Drs. Theresa Long, Samuel Sigoloff, and Peter Chambers) identified anomalous spikes in numerous diagnostic categories beginning in 2021. This precisely coincides with the mass COVID vaccination campaign among active-duty troops.
Initial DMED extracts obtained through secure access showed massive increases (compared to baseline averages from 2016–2020):
Neurological disorders ↑ 1000%+
Myocarditis and pericarditis ↑ 300%–500%
Cancers ↑ 300%+
Female infertility and menstrual irregularities ↑ 400%+
Guillain-Barré and other demyelinating disorders ↑ 600%+
These findings were publicized during a Senate hearing by attorney Tom Renz and others. They promptly reverberated through independent media, since DMED was considered one of the most reliable population-level health datasets in the world.
After the whistleblowers sounded the alarm, the DoD claimed a “data corruption issue.” Within days, the historical baselines (2016–2020) in DMED were retroactively changed, inflating prior years’ case counts to make post‑vaccine spikes appear normal.
Key facts:
The DoD did not provide verifiable documentation of how the alleged data error originated.
The original, unaltered DMED dataset, as exported by multiple credentialed physicians, remains consistent across all copies shared prior to the “correction.”
After the alteration, the database interface was taken offline for several weeks and then brought back online with the new baselines embedded.
Essentially what was first presented as a five‑fold rise across critical health conditions was digitally “normalized” away by rewriting prior year data.
Why It Mattered
Military data integrity is sacrosanct. These aren’t subjective survey data; they’re medical records logged at military treatment facilities.
The correction narrative destroyed confidence in the Defense Health Agency’s epidemiological transparency and prompted congressional inquiries into DOD data governance.
The pattern mirrored civilian analogues: VAERS underreporting, CDC spreadsheet discrepancies, and Pfizer trial data cleaning.
Independent analysts later confirmed that matching trends (neurological, cardiac, autoimmune) appeared in other military and insurance datasets not subject to DoD editing. This substantiates the whistleblowers’ claims statistically, even if DMED was altered post‑hoc.
The DMED “COVID manipulation” wasn’t simply a spreadsheet “error.” It was a reclassification and retroactive rewriting of medical reality to maintain the illusion of stability after an unprecedented physiological shock to a young, healthy population.
The moral wound is deeper than the medical data manipulation: it exposed the extent to which institutions, even military ones, will sanitize facts to preserve narratives and contracts.
Crime and Punishment
Federal Statutes that apply to the apparent data fraud that has occurred:
False Statements and Data Fabrication (18 U.S.C. § 1001)
Crime: Knowingly and willfully falsifying or concealing a material fact, or making materially false statements in any matter within U.S. government jurisdiction.
Applies to:
CDC data analysts and IT heads who approved “retroactive data corrections.”
Contractors who certified dataset validity while knowing tables were altered.
Penalty: Up to 5 years imprisonment per count, plus fines and permanent loss of federal contracting eligibility.
Obstruction of Justice (18 U.S.C. § 1505 or § 1519)
Crime: Destroying, concealing, or altering records to impede investigations or oversight.
Applies to:
Any official who deleted version‑control logs or wiped servers after congressional subpoenas.
FOIA officers who intentionally delayed or tampered with requested datasets.
Penalty: Up to 20 years imprisonment (§ 1519), forfeiture of federal pension, and evidentiary sanctions in related civil suits.
Conspiracy to Defraud the United States (18 U.S.C. § 371)
Crime: Two or more persons conspiring to impair or obstruct lawful government functions by deceit or trickery.
Applies to:
Coordinated suppression of VAERS safety signals.
Internal communications showing intent to “re‑message” data for optics.
Penalty: Up to 5 years imprisonment, plus restitution for investigative costs.
Note: DOJ often leverages § 371 as a catch‑all when proof of direct bribery or embezzlement is incomplete but collusion is evident.
Federal Program Fraud (18 U.S.C. § 666)
Crime: Theft or bribery involving programs receiving more than $10,000 in federal funds.
Applies to:
CDC grant officers authorizing duplicate or overlapping grant disbursements.
Academic intermediaries recycling program deliverables for new funding rounds.
Penalty: Up to 10 years imprisonment, restitution, and debarment from federal contracts.
Wire Fraud / Mail Fraud (18 U.S.C. § 1343 / § 1341)
Crime: Using electronic or postal communications in furtherance of a scheme to defraud.
Applies to:
Submission of falsified data or progress reports via government e‑procurement portals.
Dissemination of manipulated data summaries through official communication channels.
Penalty: Up to 20 years per count; up to 30 years if tied to public‑health emergency funding.
False Claims Act (31 U.S.C. § 3729–3733)
Nature: Civil, but treble damages + per‑claim penalties.
Targets: Grant recipients, data‑management contractors, and any official certifying compliance while knowing of falsified underlying data.
Current Status: Several whistleblower suits under seal, likely to be partially unsealed mid‑2026.
Federal Employees’ Liability Reform and Tort Compensation Act
Used to sue: Officials personally for constitutional violations, i.e., deliberate falsification depriving citizens of accurate health information under the color of law.
Aggravating Factors Raising Sentencing Exposure
Scope of Impact: Manipulation affected national vaccine policy → possible judicial “enhancement” for extraordinary societal harm.
Abuse of Trust: Courts impose harsher sentences when offenders occupy public‑trust positions (US Sentencing Guideline § 3B1.3).
Conspiracy Count Multipliers: Each coordinated misrepresentation (dataset, table, or update) constitutes a separate overt act.
Intent Evidence: Internal memos referencing “public optics,” “narrative alignment,” or “avoid vaccine hesitancy” show knowing intent, not negligence.
Summary: The Tide Has Turned
For the first time, the usual bureaucratic insulation has cracked.
The significance of this cannot be overstated: After decades of information control, federal institutions themselves are now being forced under lawful scrutiny, not just by whistleblowers, but by the government’s own enforcement arms.
After these scandals, the following reforms are needed
Mandate: real‑time monitoring of audit implementation, data transparency reforms, and whistleblower protection.
Early steps include:
Mandatory redundancy backups of all CDC databases.
Public dashboards for contractor payments.
Establishing external university partnerships for dataset verification.
Conclusion
This is yet another example of PsyWar by the Federal bureaucracy against both warfighters and the American people.
The DMED revelations and the subsequent CDC disclosures are not mere isolated incidents of error, but a unified system of institutional deception, one that places bureaucratic and institutional self‑preservation above truth. Together, these cases reveal a government‑wide mechanism designed to manufacture confidence rather than earn it. The pattern is unmistakable: when data threaten authority, the data are redefined; when truth endangers stability, stability is recast as manufactured truth.
This institutional survival instinct has metastasized into an autonomous “fraud engine,” powered by pressure, opportunity, and rationalization; the same geometry that drives corporate accounting scandals and political cover‑ups alike. Yet in this context, the stakes are immeasurably higher: the manipulation of epidemiological and medical data corrodes the very foundation of public trust and informed consent.
By choosing to curate narratives rather than confront reality, these agencies transformed science into propaganda and governance into performance. The result is an epistemic collapse; a world where facts are pliable, accountability evaporates, and truth itself becomes a controlled substance.
Unless this fraud engine is dismantled through radical transparency, immutable data systems, and independent oversight, the United States will remain ruled by institutions that no longer serve the citizen, but rather the continuity of their own illusions.
What has been revealed with the DMED and the CDC data scandals is not exceptional; it is symptomatic. It is the modern face of bureaucratic survival, deception masquerading as duty, and history will judge it as such.
If any reform is to prevent recurrence:
Immutable Data Archiving: Every dataset must have cryptographic versioning.
Separation of Analytics and Communications: Analysts cannot manage messaging.
Whistleblower Incentives: Legal immunity plus monetary reward for preserved pre‑alteration datasets.
Real‑Time Transparency: Live mirrors of all raw health data accessible to independent statisticians.
Without these, the Fraud Engine will persist eternally; pressure and rationalization are constants in human institutions.
Only removing opportunity can break the loop.
The initial report published by malone.news published Jan 03, 2026 0800h relied on an AI system (alter.systems) that generated links and information which later could not be verified. After further investigation, it became clear that the AI had fabricated some of those links and associated information. Therefore, some of the conclusions drawn were incorrect. This report has been updated to reflect those errors.
If I remember at least 2 of the three whistleblower doctors were marines. The staggering increases in obvious adverse reactions showed the devastation it was causing our armed forces. I had sent that hearing of the doctors to my primary care physician at the time, my PCP was an army reserve doctor that flew around the world injecting soldiers with the mRNA experimental vaccine. When I pressed him on the numbers he said we need to agree to disagree. It’s hard to understand doctors that obviously didn’t understand what they were pushing, pushed those chemicals anyways. I’m so glad Trump won the election which has allowed these facts to come into the light. We’re blessed he won and people like yourself Dr. Malone have finally been put in place to expose these reckless medical policies. I pray this never happens again, never again.