
Early COVID Treatment works – yet more examples
Two independent Italian teams validate earlier reports


There are many paradoxes in the COVID-19 data from the western nations concerning disease and death attributed to SARS-CoV-2 infection. One of the most problematic is the result of widespread systemic reporting bias, in which disease and deaths WITH evidence of infection are grossly over-reported as disease and deaths FROM infection by SARS-CoV-2. The truth is that we may never be able to resolve this, to get to the bottom of what really went on, due to perverse political and financial incentives to over-report COVID-19 deaths (while also minimizing toxicity of the vaccines). But there is no question that if you are admitted to a western hospital with a COVID-19 diagnosis, your risk of death during that hospitalization has been amazingly high.
In my opinion, many of those hospital deaths were avoidable – many were iatrogenic (due to medical error). Iatrogenic disease is the result of diagnostic and therapeutic procedures undertaken on a patient. Again and again I hear academics, physicians, hospitalists and relatives of patients speak of the horrors of hospital-based treatment of COVID-19, of the unnecessary isolation of the patients, of the horrible and inhumane treatment which patients are receiving, of the toxicity of the FDA-approved and Fauci-promoted drug Remdesivir (globally nicknamed by nurses and orderlies “run, death is near”), and of the contribution of bad intubation and ventilation practices to those outcomes.
But they never, ever acknowledge that their mismanagement of these patients has contributed to the death toll. The hospitalists have often slavishly followed the inpatient guidance protocols of the NIH (which has never before been in the business of setting national treatment standards), while failing to even be willing to try the alternative inpatient and outpatient treatments which many independent physicians have developed and successfully implemented while saving many thousands of patients’ lives. Clearly, what is needed is a way to keep patients from ever getting to the hospital and receiving these dysfunctional treatments associated with high levels of iatrogenic disease and death.
There is no question in my mind that early COVID-19 treatment saves lives, and many different repurposed drug treatment protocols for treating this disease have become popular despite withering criticism and gaslighting from FDA, NIH, corporate media and hospitalist physicians. For example treatment protocols, see those developed by FLCCC, Dr. Vladimir Zelenko, Drs. George Fareed and Brian Tyson , and the European doctors who practice under the banner of Ippocrateorg.org. In just one example, while in the USA Ivermectin has been vilified by both FDA and the press, worldwide adoption of Ivermectin for treatment of COVID-19 disease is now at 45%!
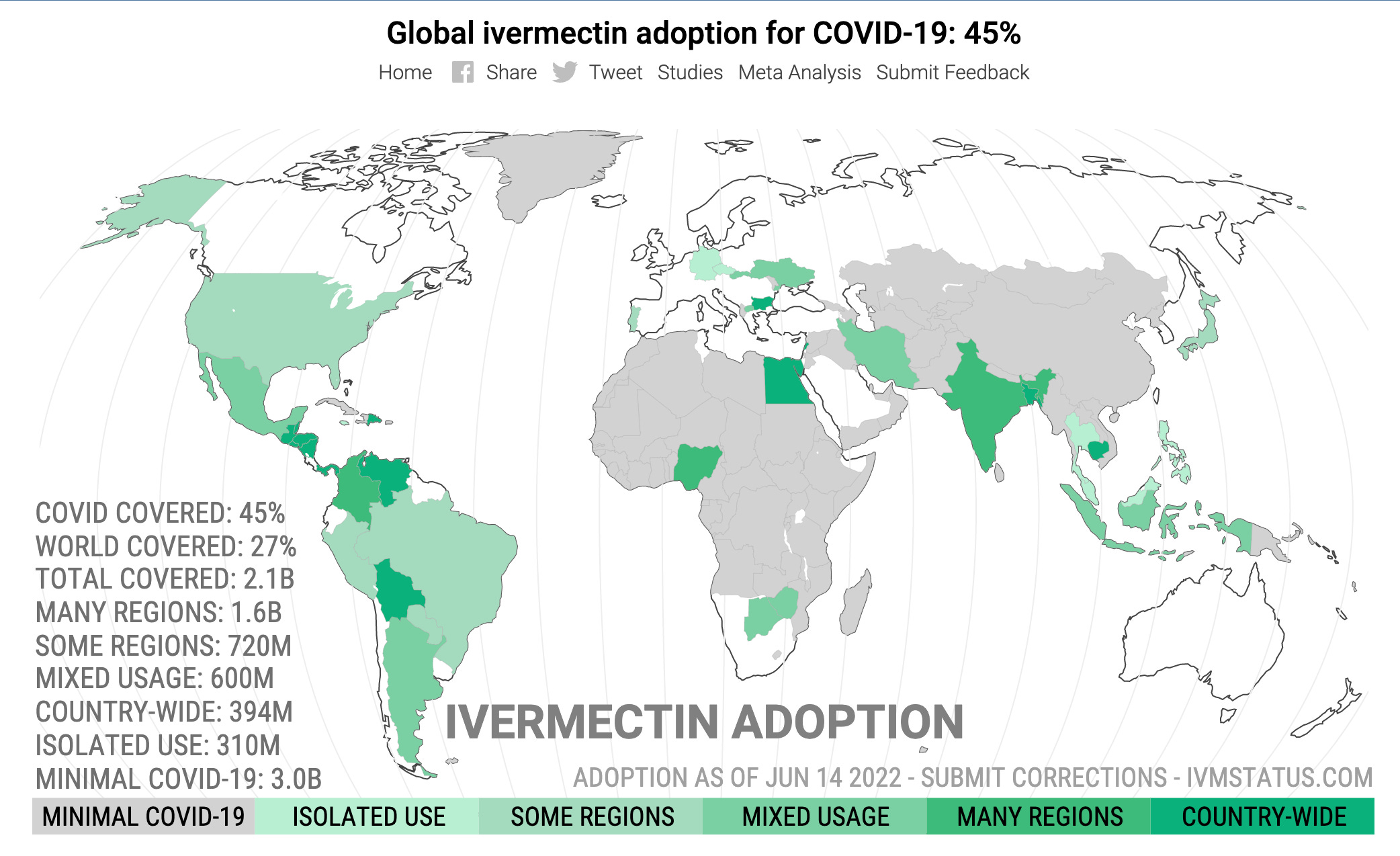
Ivermectin is currently used for about 27% of the world's population. Countries where COVID-19 mortality is close to zero may not have incentive to adopt treatments. When excluding these countries, ivermectin adoption is about 45%. We excluded countries where the cumulative mortality over the preceding month was less than 1 in 1 million, according to the data at https://ourworldindata.org/). For the estimated population coverage, isolated use, some regions, mixed usage, and many regions use a factor of 0.05, 0.25, 0.5, and 0.75 respectively. For source reference, please see here.
While many of these alternative early treatment and hospital treatment protocols rely on drug combinations which typically include Hydroxychloroquine + Azithromycin (the combo championed by Dr. Didier Raoult) or Ivermectin, there are many other drugs and combinations which have shown substantial efficacy in both outpatient and inpatient treatment environments.
For example, those who have followed my work over the last two years may be familiar with the data supporting the use of Famotidine with or without Celecoxib. For relevant papers, please see here, and here, and here. Unfortunately, despite passing peer review, publication of much of this work and associated findings was actively blocked by various academic journals and ridiculed by lay press including the Washington Post (see also here), despite having been demonstrated to have benefits in clinical trials including a randomized Phase 2 clinical trial. More detail on that sordid story in a future article, but how and why journalists with no medical training working for the Washington Post became arbiters of medical truth continues to elude me. Who knows how many lives could have been saved if the lay press had just focused on doing solid reporting rather than trying to influence clinical treatment practices while attacking physicians that were just trying to do their jobs.
Although it may seem like both the government and the lay press in the United States has been particularly hostile to early treatment protocols employing cheap generic drugs for COVID-19, things have been even more difficult for Italian physicians providing early treatment. This makes the following studies even more remarkable!
An Italian team working in a traditional hospital setting has published two peer reviewed studies, one in the Lancet-affiliated journal eClinical Medicine and the other in Frontiers in Medicine. The clinical treatment protocol tested in the clinical trial associated with these publications is built around COX-2 inhibitors (Nimesulide, which is available in EU but not USA or Celecoxib, which is available in both EU and USA). In the case of either of these agents being contraindicated due to patient pre-existing conditions, the combined COX-1 and COX-2 inhibitor Aspirin (careful, this is also used to treat horses…) was substituted. The title of the corresponding clinical trial says it all-
“A Simple Approach to Prevent Hospitalization for COVID-19 Patients”
Here is the resulting recommended outpatient clinical treatment protocol-
I. Non-steroidal anti-inflammatory drugs (NSAIDs)
Relatively selective COX-2 inhibitors §# (for myalgias and/or arthralgias or other painful symptoms)
§ based on the ratio of concentrations of the various NSAIDs required to inhibit the activity of COX-1 and COX-2 by 50 percent (IC50) in whole blood assays
#unless contraindicated
Nimesulide *
100 mg b.i.d p.o, after a meal, for a maximum of 12 days.
Or
Celecoxib *
Initial oral dose of 400 mg, followed by a second dose of 200 mg on the first day of therapy. In the following days, up to a maximum of 400 mg (200 mg twice a day) should be given as needed for a maximum of 12 days
* Should the patient have a fever (≥37.3°C) or develop laboratory signs of hepatotoxicity associated with nimesulide, or if there are contraindications to celecoxib, these drugs should be substituted with aspirin (a COX-1 and COX-2 inhibitor) (500 mg twice a day p.o.—after a meal). Patients receiving these treatments should also be given a proton pump inhibitor (e.g., lansoprazole-−30 mg/day; or omeprazole-−20 mg/day; or pantoprazole-−20 mg/day).
Approximately 3 days after the onset of symptoms (or longer if the physician is seeing the patient for the first time), a series of hematochemical tests should be performed (blood cell count, D-dimer, CRP, creatinine, fasting blood glucose, ALT). Nimesulide/celecoxib (or aspirin) treatment can continue if inflammatory indexes (CRP, neutrophil count), ALT, and D-dimer are in the normal range,.
II. Corticosteroids*
Dexamethasone (for persistent fever or musculoskeletal pain or if hematochemical tests are repeated a few days later and there is even a mild increase in the inflammatory indexes—CRP, neutrophil count –, or if the patient has a cough and oxygen saturation (SpO2)<94–92% occur)
8 mg p.o. for 3 days, then tapered to 4 mg for a further 3 days, and then to 2 mg for 3 days. This makes a total of 42 mg dexamethasone over 9 days.
*The duration of corticosteroid treatment also depends on the clinical evolution of the disease
III. Anticoagulants
Low−molecularweight(LMW)heparin* (when the hematochemical tests show even a mild increase in D-dimer, or for thromboembolism prophylaxis for bedridden patients)
Enoxaparin, at the prophylactic daily dose of 4,000 U.I subcutaneously—i.e., 40 mg enoxaparin. Treatment recommended for at least 7–14 days, independently of the patient recovering mobility.
*unless contraindicated (e.g., ongoing bleeding or platelet count<25 × 109/L)
IV. Oxygen therapy
Gentle oxygen supply in the early phase of the disease, possibly before pulmonary symptoms manifest, in the presence of progressively decreasing oxygen saturation—as indicated by an oximeter—or following a first episode of dyspnoea or wheezing.
Conventional oxygen therapy is suggested when the respiratory rate is >14/min and oxygen saturation (SpO2) < 94–92%, but is required with SpO2 <90% at room air. With liquid oxygen, start with 8–10 liter/min and monitor SpO2 every 3–4 h. Titrate oxygen flow rate to reach target SpO2 >94%. Then the rate of oxygen administration can be reduced to 4–5 liter/min (but continue SpO2 monitoring every 3–4 h). With gaseous O2, start with 2.5–3.0 liter/min, but monitor SpO2 more frequently than with liquid oxygen, and titrate flow rates to reach target SpO2 >94%. Hospitalization could be considered, if feasible, when oxygen saturation (SpO2) ≤ 90% at room air, despite conventional oxygen therapy.
V. Antibiotics
Azithromycin* (with bacterial pneumonia or suspected secondary bacterial upper respiratory tract infections, or when hematochemical inflammatory indexes (CRP, neutrophil count) are markedly altered)
500 mg/day p.o. for 6–10 days depending on the clinical judgement
* Should the patient be at risk of or have a history of cardiac arrhythmia or present other contraindications, cefixime (400 mg/day p.o for 6–10 days) or amoxicillin/clavulanic acid (1 gr three times a day for 6–10 days) can be considered as alternatives to azithromycin.
In a separate study completed by the IppocrateOrg Association Working Group for the Early Outpatient Treatment of COVID-19 (which is predominantly an association of Italian physicians and scientists), an alternative protocol also demonstrated effectiveness in outpatient treatment of COVID-19.
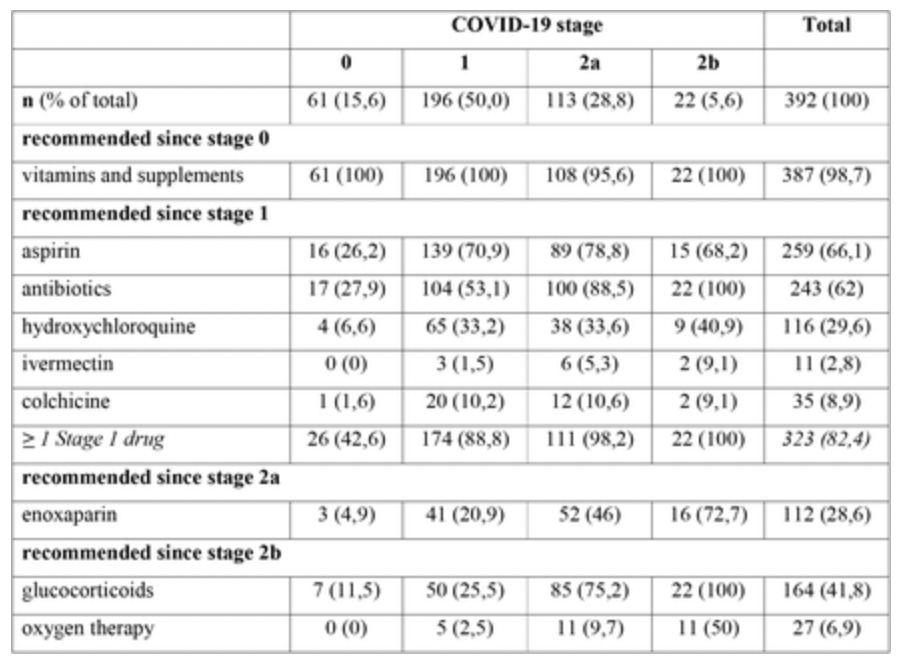
EARLY OUTPATIENT TREATMENT OF COVID-19: A RETROSPECTIVE ANALYSIS OF 392 CASES IN ITALY
These researchers conclude:
“This is the first study describing attitudes and behaviors of physicians caring for COVID-19 outpatients, and the effectiveness and safety of COVID-19 early treatment in the real world. COVID-19 lethality in our cohort was 0,2%, while the overall COVID-19 lethality in Italy in the same period was between 3% and 3,8%. The use of individual drugs and drug combinations described in this study appears therefore effective and safe, as indicated by the few and mild ADR reported. Present evidence should be carefully considered by physicians caring for COVID-19 patients as well as by political decision makers managing the current global crisis.”
The protocol used for this study is more typical of the protocols used in the United States. As is often the case in the United States, the general treatment protocol developed by the Ippocrateorg team is staged by disease severity, and can be found here.
A summary table of the treatment received for the 392 summarized Italian cases is appended below (note the use of aspirin):
In conclusion, irrespective of the excess death and disease associated with the mandated genetic vaccines, there is no doubt in my mind that the concerted and coordinated propaganda and information control efforts of the United States Government Department of Health and Human Services, acting in alignment and as sponsors of Big Tech and Corporate Media censorship, have cost large amounts of unnecessary death and disease due to both iatrogenic causes during hospitalization as well as by suppression of life saving early treatment protocols. The data supporting this conclusion increase almost daily. The unresolved issue remains. Will anyone be held accountable for this avoidable tragedy?

The failure of doctors to aggressively treat COVID in the early stages is a huge scandal. I just had a moderate (7-day) bout with COVID. The doctor would not "prescribe" anything but ibuprofen. Luckily I knew enough to self-administer the protocol: IVM, Quercitin, Vit D3, zinc, aspirin, etc. I'm fine.
Doctor Malone, we deeply appreciate your tireless work.
The breadth and depth of the criminality around this issue never ceases to amaze me. I honestly cannot even imagine who or what one can appeal to for justice. Every - EVERY - institution in this failed state is corrupt and in on the plan/narrative, it appears. Sad and depressing.