
Measles Returns: A Texas Death and the Debate Over Medical Response
An investigative journalism report by Trial Site News


Measles Returns: A Texas Death and the Debate Over Medical Response
Initially Published by Trial Site News. Republished by permission.
Apr. 9, 2025, 8:30 p.m.
In an episode of Good Morning CHD, a critical care doctor and known celebrity of the medical freedom movement Dr. Pierre Kory, and Brian Hooker, Chief Scientific Officer at Children's Health Defense (CHD), discussed the death of an unvaccinated 8-year-old child, named Daisy Hildebrand, who tragically passed away following a measles infection according to the Texas Department of State Health Services (DSHS). Kory pointed out that this incident occurred at the same hospital where another child had died previously from measles complications. In a bombshell revelation he emphasized that the hospital’s handling of the case may have contributed to both deaths. This recent event concerned the argument that the death was not due to the measles virus itself, despite what Texas authorities have implied in carefully worded press releases, but due to systemic medical care errors. This episode raises wider questions regarding vaccine safety, perceived measles vaccination risk, and public health policy roles in averting such fatalities, not to mention the quality of care in at least one major hospital in Texas. If the Texas Health and Human Services press release proves to be inaccurate, could this also represent an attempted manipulation of the public? Could this point to a deliberate cover-up?
The stakes don’t get bigger in the world of health. With a measles outbreak flaring up in Texas, vaccine skepticism is on the rise since government overreach during the COVID-19 pandemic. Study after study shows that the MMR vaccine protects the population. Even when so-called breakthrough infections occur, they tend to be far more mild as one recent investigation demonstrates.
But certainly, vaccine skepticism may worsen if public health agencies are caught manipulating messaging to heighten fear. In the CHD event, Dr. Kory goes on the record, essentially declaring that not only the hospital involved, but that the State’s health agency appears to be spinning the news to imply measles was the prime culprit.
Dr. Robert Malone covered this topic, also prodding TrialSite to investigate this affair deeper.
In its April 6, 2025, news release, the Texas DSHS announced the death of a school-aged, unvaccinated child who had tested positive for measles and was hospitalized in Lubbock. The state reports the child had no known underlying health conditions and died of what doctors described as “measles pulmonary failure,” marking it as the second death in Texas's current measles outbreak, which has tallied 481 confirmed cases as of April 4.
While DSHS does not explicitly state that measles was the sole cause of death, the language strongly implies it played a direct and primary role. The release also reiterates that measles can lead to severe complications including pneumonia and death, particularly in unvaccinated individuals.
Accessing the death certificate would be key, and to date, this is not available.
Analysis of the Second Measles Death
In the case of Texas’s second reported measles-related child death, Dr. Pierre Kory argues the tragedy was not directly caused by the virus itself but rather by systemic medical mismanagement. After reviewing the medical records, Kory asserts the child’s death was preventable and resulted from serious failures in care, not the measles infection per se. He raises concerns that the child’s unvaccinated status may have influenced the quality and urgency of treatment, pointing to potential bias within the healthcare system.
Kory contends that while measles is often portrayed as inherently dangerous and potentially fatal, in this case, delayed or improper treatment played a larger role in the outcome. This challenges the conventional narrative that attributes such deaths as linked to measles and raises difficult questions about how unvaccinated patients are treated during outbreaks. The case underscores the ethical and clinical complexities surrounding measles management, vaccine choice, and equitable care standards.
Arguments Against Measles Vaccination
In the entire video, Kory and CHD lead scientist Brian Hooker present a doubtful view of the global emphasis on measles vaccination, questioning its necessity and effectiveness in preventing deaths from the disease. He argues that measles, while certainly a serious disease, has throughout history been overblown in its natural danger. Dr. Kory suggests that the vaccine, although widely considered a key tool in controlling the disease, might not be as crucial as it is often portrayed, particularly when it comes to the effectiveness of medical treatments for those who do contract the virus. A large body of evidence contradicts these statements, and in fact, even Robert F. Kennedy Jr. has gone on the record during the measles outbreak of the importance of vaccination.
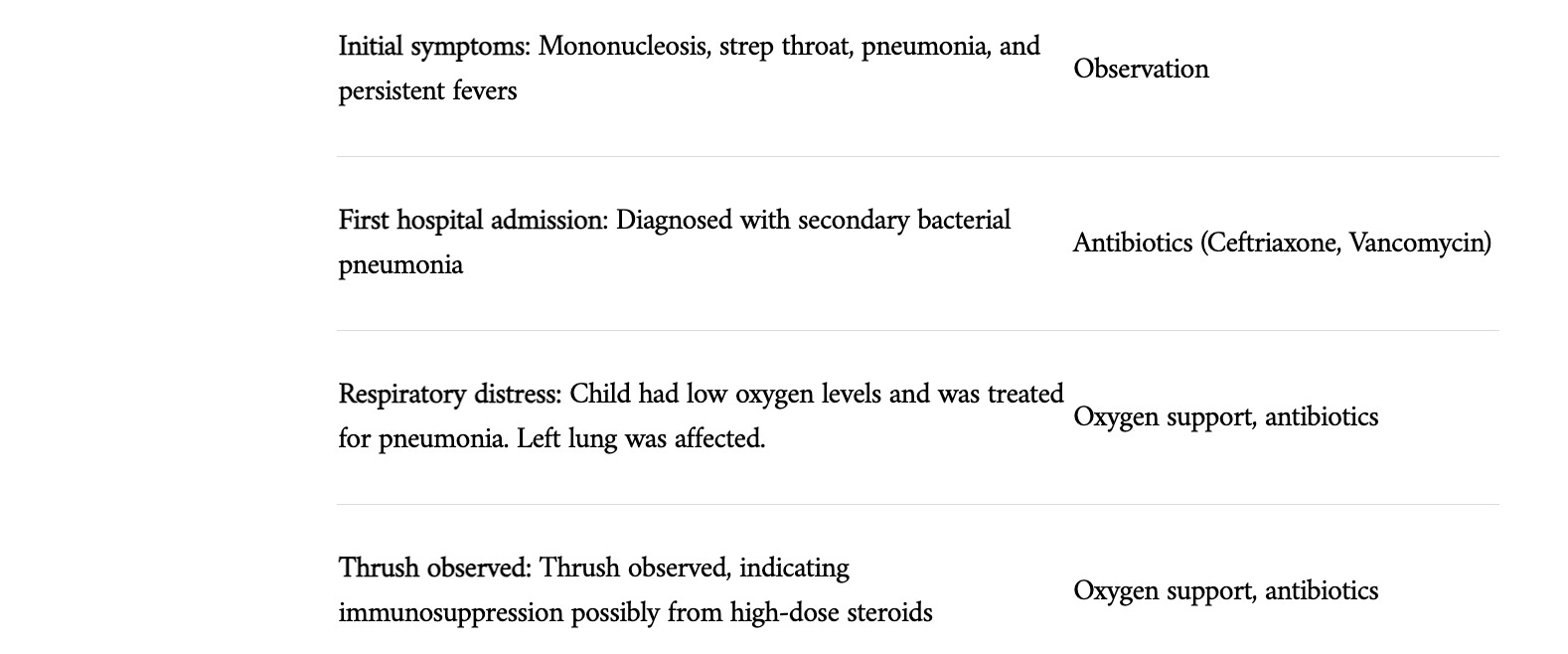
Kory states that he was able to access the medical records of Daisy Hildebrand, who had previously been healthy until about a month before the initial hospitalization. According to Kory, she initially developed mononucleosis, followed by strep throat and then pneumonia. Her condition seemingly did not improve, and she remained ill with recurring fevers that would not subside. Upon her first hospital admission, she was diagnosed with secondary bacterial pneumonia. During this visit, thrush was observed in her, indicating immunosuppression likely due to high-dose steroids that she had been administered for her prior illnesses.
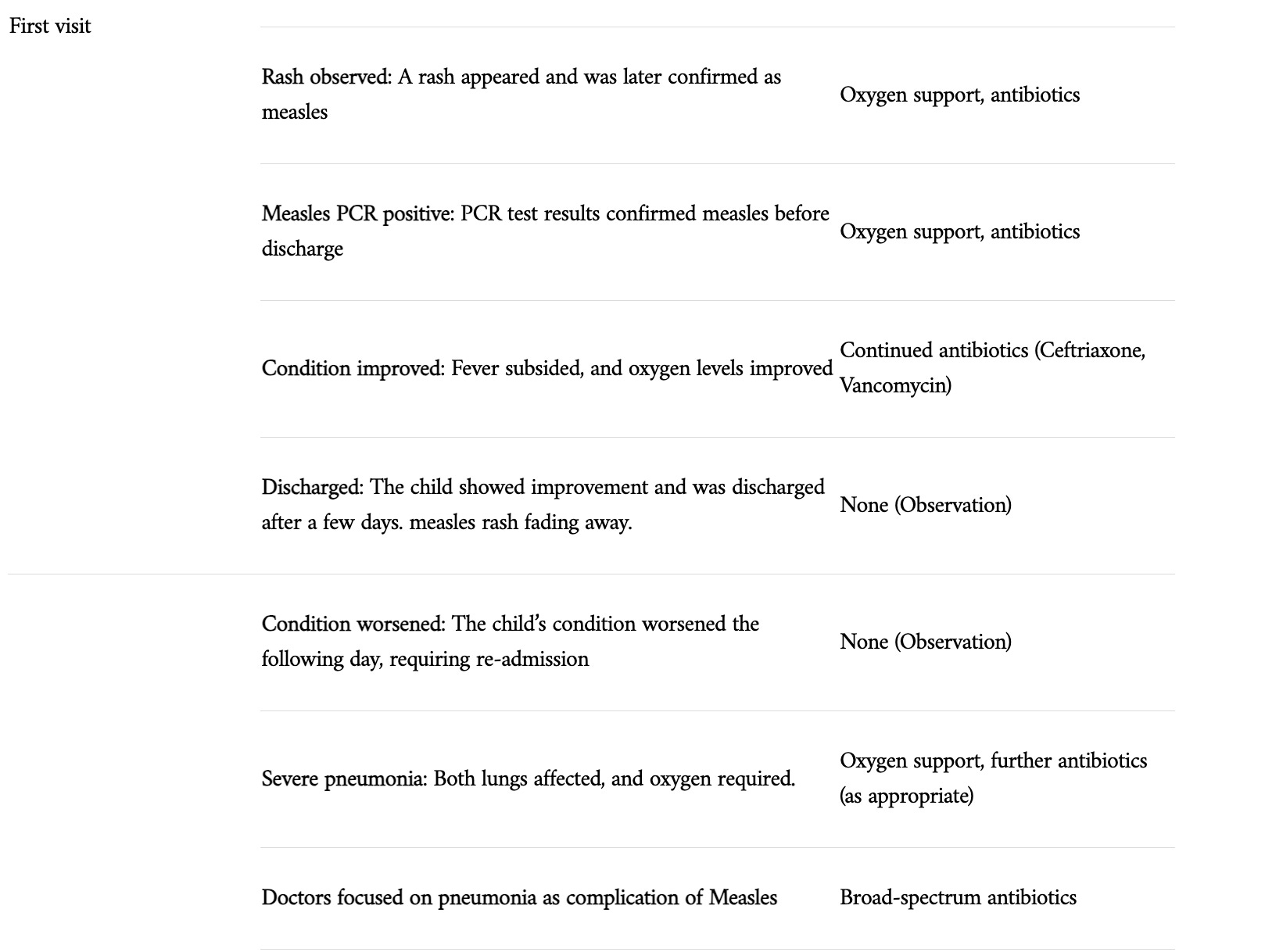
For the pneumonia, she received antibiotics (ceftriaxone and vancomycin) which deviated from the standard treatment for pneumonia. While this antibiotic regimen was not ideal, it yielded some improvement, and she showed signs of recovery. She was discharged after a few days, but the following day, her condition worsened, leading to a second hospitalization. Upon admission for the second time, she was in a much worse state, with both lungs affected and requiring significantly more oxygen.
While it is not 100% clear when she was first diagnosed with Measles, Kory states that she had a positive Measles test during her first hospital stay, but at the time of her discharge, the rash was clearing up and her overall condition had improved.
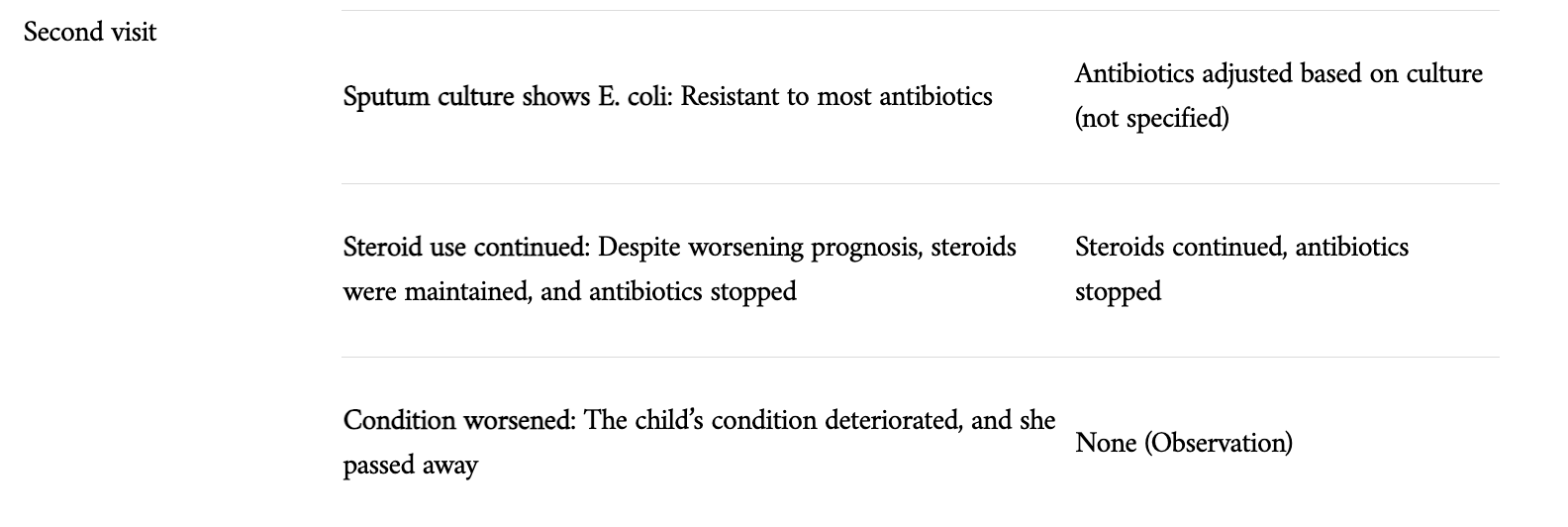
According to Kory, the healthcare team’s approach to her condition became particularly problematic during the second hospitalization. The hospital doctors assumed the pneumonia was a measles-related pneumonia and thus delayed proper treatment further. Dr. Kory criticizes this approach, pointing out that hospital-acquired pneumonia (HAP) should have been considered, especially given her recent ICU stay and immunosuppressive state. Instead, the doctors did not fully extend their coverage of antibiotics, which led to a slow decline. It was not until after days that a sputum culture was dispatched, showing an E. coli infection resistant to most antibiotics. Unfortunately, by that point, it was too late.
What follows is a timeline of the events according to Kory’s interpretation as presented to CHD:

While Dr. Kory questions the necessity of vaccination, his primary concern in this case revolves around medical mismanagement. In his view, the child's death was not due to measles, but rather the result of significant oversights by the medical team. Again, the State in its press release, heavily implies the death was linked to complications from a primary measles infection in a young girl who was unvaccinated.
Discrepancy in Diagnoses: Measles or Something Else?
Both the hospital and at least state officials via a press release implied that the child died due to pneumonia as a complication of Measles, yet Kory and the CHD team challenges this conclusion, asserting that the child did not die from Measles, but rather from a hospital-acquired bacterial infection (E. coli), which was misdiagnosed as a pneumonia from measles and mistreated. While the child tested positive for measles, Kory states the focus on measles led to the oversight of a more serious and treatable condition, which ultimately led to the child’s tragic death.
Further complicating the situation is the discrepancy regarding the measles rash. The parents of the child did not observe the rash, yet doctors in the hospital claimed to have seen it. This conflicting testimony raises significant questions about the accuracy of the observations and whether the rash was as prominent as reported. Dr. Kory, in his review, pointed out that the rash, which was eventually confirmed as measles, may not have been immediately visible or prominent enough for the parents to notice. Also, he pointed out that the description of the rash was inconsistent through the chart. Despite the PCR test confirming measles, Dr. Kory’s position remains that a hospital-acquired bacterial infection was the true cause of death.
What does the Hospital and State have to Say?
TrialSite reached out to both the hospital and the State of Texas. TrialSite both left messages and sent an email to Aaron Davis, Vice President and Chief Experience Officer for UMC Health System. As of this writing Ms. Davis has not responded to TrialSite’s outreach.
TrialSite also reached out to Chris Van Deusen, Director of Media Relations, Texas Department of State Health Services.
A Senior Press Officer Lara Anton responded with an email that did not help us get to the bottom of this. According to Ms. Anton in her email to TrialSite publisher Daniel O’Connor:
“Hi Daniel
The health department is prohibited by law from sharing a person’s medical record. DSHS also cannot share information that could be used to identify a specific person. The information in the news release came from the child’s doctors, who determined the cause of death (standard practice in Texas). You’ll notice that the news release does not include any specific details about the child and no details about treatment because we are prohibited from sharing that information. The health department does not regulate the practice of medicine. The Texas Medical Board is the regulatory agency for that.”
So, neither the State nor the hospital seem to want to communicate any material information at this point—at least not with TrialSite.
Plus, Trialsite also has no reason to believe that the state nor the child’s doctors are misrepresenting the child’s diagnosis, prognosis or treatment, and is only here to point out the glaring discrepancies between the press release and a medical doctor’s subsequent review of the child’s medical records.
Trialsite understands the seriousness of medical mismanagement accusations and only pursues clarity surrounding the child’s tragic death. Given the charged climate around childhood vaccination, Trialsite feels an independent review of the medical records would be the best path forward.
A Challenge to the Measles Narrative: A Call for Medical Accountability Beyond Vaccination:
CHD and Dr. Pierre Kory’s blistering critique of the medical handling in the second Texas measles death cuts against the grain of dominant public health narratives. Far from blaming measles alone, Kory lays the child’s death at the feet of clinical mismanagement—misdiagnosed hospital-acquired pneumonia, premature cessation of antibiotics, and continued use of high-dose steroids despite signs of systemic infection. His analysis reframes the tragedy not as a cautionary tale about vaccination refusal, but as a failure of medical vigilance and a warning about the dangers of tunnel vision in healthcare when vaccination status eclipses diagnostic diligence.
This isn’t just a case critique—it’s a challenge to the scaffolding of modern vaccine-centric public health. Kory doesn’t dismiss vaccines outright; instead, he demands they not be treated as singular solutions. In his view, the obsession with immunization metrics has come at the expense of clinical care quality.
He calls for a rebalancing, meaning a prevention model that pairs immunization with robust treatment infrastructure, diagnostic agility, and equitable care for all patients, vaccinated or not. Without this, the doctor and his colleagues at CHD warn that vaccine campaigns risk becoming hollow gestures, propped up by a system that fails patients at their most vulnerable.
But outbreaks don’t just fail patients, they strain entire systems. The consequences of inadequate vaccination stretch far beyond individual risk: they reverberate through emergency rooms, pediatric ICUs, and resource-starved clinics. When preventable diseases resurge, they soak up capacity, redirect personnel, and force triage decisions no doctor wants to make. In the worst-case scenario, they collapse the very scaffolding they’re meant to test.
In a time when vaccine hesitancy is already fraying trust in institutions, and measles is spreading with over 50 hospitalizations in Texas alone and cases and hospitalizations documented in other states, Kory’s intervention is both combustible and consequential. Should the doctor be correct, it exposes an uncomfortable truth: that medical systems, too, must be held to account—not just individuals who forgo a shot. If his claims hold water, they suggest that the real path to health security lies not in doubling down on singular solutions but in building a healthcare system as resilient, responsive, and multifaceted as the diseases it aims to defeat.
In light of Kory’s serious allegations, an independent review of the child’s medical records and death certificate is not only warranted—it is essential. If public health officials continue to attribute, or at least imply in press releases, deaths solely to measles without scrutinizing the quality of medical care provided, they risk eroding public trust in their institutions. But again, we hope for independent verification, free from biases as much as humanly possible.
TrialSite will continue to investigate, seeking the death certificate as well as any other material facts that can help shine more light on this case.
Transparency, accountability, and a willingness to re-examine outcomes—especially when clinicians raise red flags—are foundational to restoring confidence in both vaccine policy and healthcare delivery.
Frankly, the stakes are high. When preventable deaths are politicized or mischaracterized, the entire architecture of public health credibility begins to falter. We had enough of that during COVID-19, it cannot continue.
As a middle child in a family of 8 kids, I had every childhood infection… measles at 18 months old and extremely ill, on to chicken pox, mumps-bilateral, German measles, scarlet fever and multiple episodes of strep tonsillitis.. until they were removed at age 14. I went onto nursing school and then worked 40 years in the Emergency Room. I never caught the flu, gastrointestinal issues etc, despite not taking any vaccines against the virus’s. Due to hospital policies, my last 3 years of employment, I had to take the flu vax against my wishes. All staff around me(most younger) got the flu multiple times… yet I never did. I always believed that my robust immunity was the result of all of my childhood illnesses and served me well as an adult in healthcare!
All I remember about being sick was we all had to wear sunglasses at one time or the other. We all had measles, mumps, flu, whatever. I would not wish illness on anyone for sure. We survived. Like a person beside me I talked with when donating blood, he said, we're not supposed to be sick anymore. Think about that. Personally, I would say that all these efforts to make us "healthy" are actually making us perpetually sick.