
Medical Guilds are Bad Medicine
Monopolies, Oligarchy, Elitism, Authoritarianism and Groupthink are hurting patients, driving up costs, blocking innovation, and trampling civil rights


Restored Medieval Guild Halls at Grand Place, Brussels
In a broad, metaphorical sense (as often used by economists like Milton Friedman or in historical analyses), the term “guild” refers to professional organizations and regulatory bodies that function like traditional medieval guilds by controlling entry into the profession, setting standards, influencing licensing, and protecting members’ economic interests. Common examples of Medical guilds include:
State Medical Boards. They are empowered by individual states to regulate licensing and discipline physicians (the closest to actual “guild-like” control over who can practice). During COVID, state medical boards became notorious for de-licensing physicians for not complying with arbitrary and capricious “standard of care” guidelines promoted by Dr. Anthony Fauci, the CDC (Rochelle Walinski and Dimitri Dasalakis), and the FDA (Janet Woodcock, Peter Marks).
American Medical Association (AMA). The largest and most influential physician organization, sometimes described as a “guild” due to its historical role in limiting physician supply and shaping reimbursement policies
American Academy of Pediatrics (AAP). During COVID, was a leading advocate for masking children down to six months of age, and promoted gene therapy-based vaccination despite clear evidence of significant life-threatening myocarditis risk and extremely low pediatric COVID risk. Actively advocates that AAP members “fire” patients who are not fully compliant with AAP-endorsed vaccine schedules. Actively advocates for “cocooning”, requiring grandparents and relatives to be revaccinated for common childhood illnesses before being allowed to visit newborn children. Actively advocates for “gender affirming care” and “gender reassignment surgery” for children.
American Dental Association (ADA) — Similarly functions with strong professional control in dentistry
In modern usage, most people refer to these as professional medical associations or specialty societies rather than “guilds.” Still, the guild analogy persists in discussions of professional self-regulation and barriers to entry because the documented monopolistic behavior of these organizations is very similar to the anti-competitive excesses associated with the Guild-controlled economies of Europe from the Middle Ages to the early stages of the Industrial Revolution.
The disruptive, transformational culture of innovation and mass production finally broke the centuries-long economic hold of the Guilds, which played a key role in developing and organizing the European cities and States that arose during the Middle Ages. One of the most famous artifacts of the era of the Guilds can be seen at Grand Place in Belgium (just a short walk from the modern building that houses the European Union), where each elaborate building was built and owned by one of the powerful trade guilds that dominated the European economy at the time, serving as a physical reminder of the economic power and influence of the Guild that occupied each building.

Headquarters of the American Academy of Pediatrics (AAP), 183,603 square feet, Itasca, IL, completed in 2017 at a cost of $47,356,708. Annual revenue of the AAP is approximately 75M$.

Headquarters of the American Medical Association (AMA), a 52-story skyscraper in downtown Chicago, is located at 330 North Wabash Avenue, Suite 39300, and is known as AMA Plaza. The AMA leases floors 39-47 (265,000 square feet) at an annual cost of approximately 7-8M$. Annual revenue for the AMA is approximately 500M$.
What is a Guild?
In the most generous and benign sense, a Guild is a group of people who band together because they do the same kind of work, share common interests, or want to achieve something together. The meaning changes quite a bit depending on the context. Historically, Guilds have often been associated with a variety of self-serving, monopolistic, anti-competitive, and anti-innovative behaviors.
In medieval Europe (roughly 11th–16th centuries), a guild was an influential professional association of craftsmen, artisans, or merchants of the same trade (e.g., blacksmiths, weavers, bakers, cabinetmakers, goldsmiths, merchants). Functionally, medieval guilds operated as a combination of a modern trade union, professional licensing board, cartel/quality control mafia, and social club/mutual aid society. Medieval guilds controlled who could work in the trade in a city (you usually had to join the guild), and often were a significant source of political power in city governments. Essentially operating as regional monopolies, the Guilds set quality standards, regulated prices & limited competition, provided training through an enforced system of apprentices, journeymen, and then eventually masters (the famous career ladder), and protected members by providing sick pay, widows’ & orphans ’ funds, funerals, and other membership benefits.
The Medieval guilds were extremely influential until the rise of centralized States and early capitalism began dismantling them in the 17th–19th centuries. This challenges the narrative that all monopolies are the creation of the State. The monopolistic Guild structure predated the rise of the modern Nation-State and became a fundamental organizational force, playing a significant role in the rise of major European cities and Nation-States.
The structure and function of Medieval Guilds is almost a precise analog to present-day American medical Guilds, except that medieval guilds did not rely on publications to communicate norms, expectations, and standards of practice (ergo, “Journal of the American Medical Association”).
The printing press was a relatively recent invention, and printing had not become widespread. Instead, their internal communication and record-keeping relied on handwritten manuscripts. These were not periodically distributed like newsletters; they were official records kept in the guildhall for consultation by officers (e.g., masters, wardens) or read aloud at assemblies.
Medieval Guilds emphasized oral traditions, in-person gatherings (e.g., feasts, processions, masses), and hierarchical control; information flowed top-down through masters and officials, not through mass-distributed publications. Members might hear rules announced verbally during meetings, feasts, or religious services rather than receive personal copies.
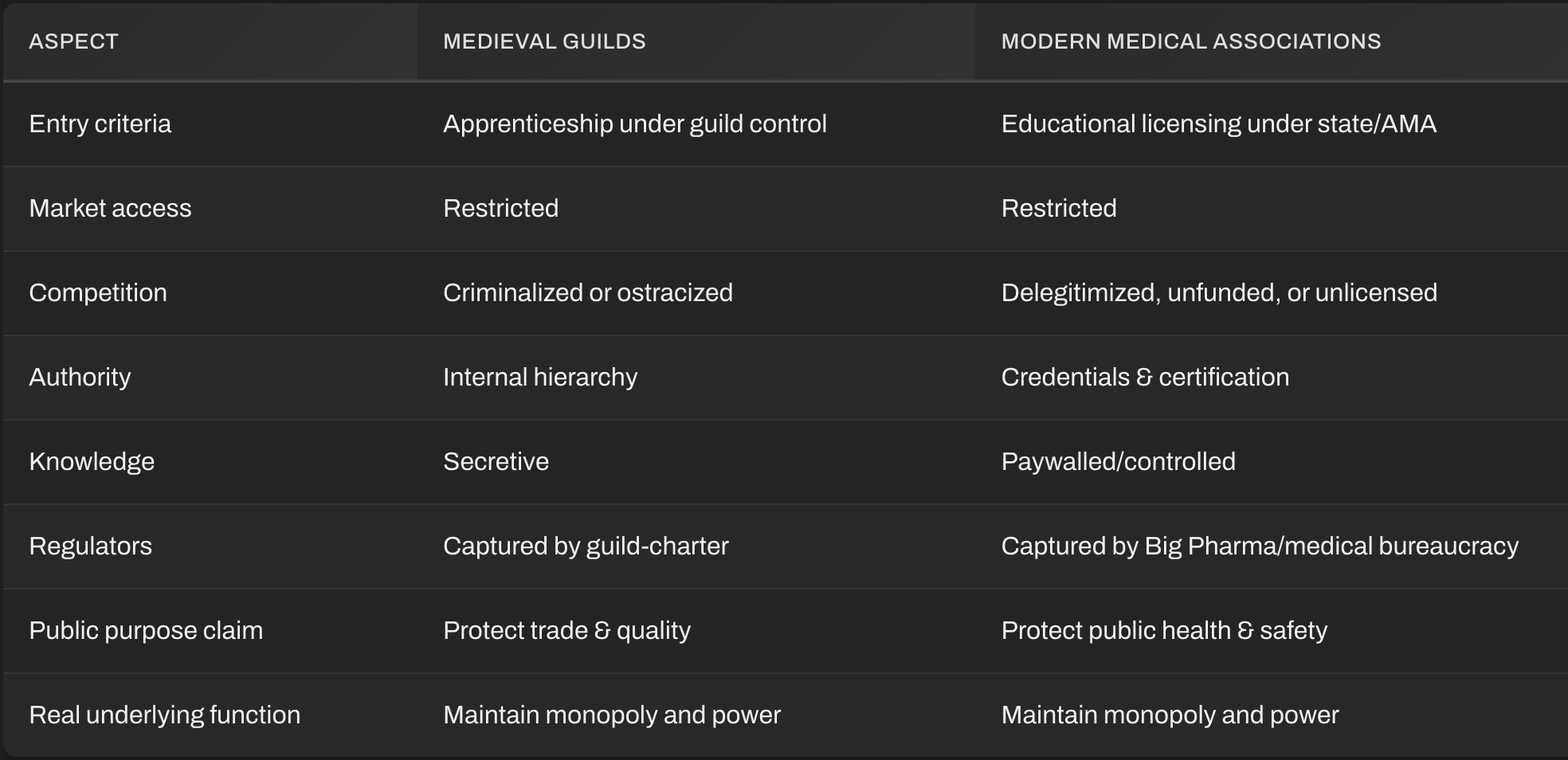
Characteristics shared between Medieval Guilds and present-day American medical Guilds include the following:
Exclusive monopolies on a defined area of practice (control of entry)
A formalized apprentice–journeyman–master path (internship, residency, fellowship, certification)
Price & quality regulation (often reinforced through lobbying and influence campaigns targeting insurance companies and the Federal Government)- Suppression of competition, price fixing.
Establishment and exploitation of political power.
The ability to censor, punish, and intimidate dissenting points of view within the guild members.
Control of Entry
Medieval Guilds:
You couldn’t just decide to start smithing swords or brewing ale. Membership was tightly controlled. To practice, you had to go through years of apprenticeship under the guild’s oversight, pay dues, and be approved by senior members.Modern Medical Associations (e.g., AMA, AAP, state boards):
The medical establishment likewise enforces limited entry through lengthy, expensive credentialing pathways, board certifications, licensing exams, and postgraduate requirements. The stated goal is to maintain competence, but the practical result is inflation of entry barriers and suppression of rival paradigms (e.g., naturopaths, osteopaths, holistic or functional practitioners).
In both cases, control of entry ensures a scarcity of practitioners, and scarcity sustains high prices.
Suppression of Competition
Medieval Guilds:
Guilds often lobbied local authorities to ban non-guild artisans, seize tools from unlicensed craftsmen, or impose fines.Medical Institutions:
The AMA historically lobbied to criminalize or delegitimize alternative medical practices (chiropractic, herbalism, midwifery, homeopathy, etc.) and continues to influence legislation determining who can legally practice medicine. Even today, innovative treatments or research outside institutional orthodoxy face funding denial, professional ostracism, and media dismissal.
Both systems framed (and continue to frame) outsiders not as competitors but as “charlatans” — a moral framing to justify economic exclusion.
Price Fixing and Economic Protectionism
Medieval Guilds:
Set uniform prices, controlled production standards, and punished undercutters.Modern Medicine:
Price coordination is officially prohibited, yet institutional monopolies and insurance networks produce the same effect indirectly. CPT coding (created by the AMA), “standard of care” boards, and insurer-medical agreements effectively fix what kinds of treatment are financially viable. Physicians who work outside that matrix can’t be reimbursed and are marginalized.
The AMA’s control of CPT billing codes is directly comparable to a medieval guild controlling the ledger of what’s a legitimate trade.
Credentialism as Authority
Medieval Guilds:
Status — apprentice, journeyman, master — defined social legitimacy.Medical Associations:
Degrees, board certifications, and memberships define who is an “expert.” Institutional validation substitutes for actual track record or outcomes, just as medieval masters were treated as authorities regardless of individual skill variation.
This creates a priestly hierarchy — credentialing as a form of secular anointment.
Paternalistic Monopoly on Knowledge
Medieval Guilds:
Guarded trade secrets; apprentices were forbidden to share them.Medical Institutions:
Control modern biomedical “trade secrets” through paywalled academic publishing, exclusive research funding, and intellectual property protection. Clinical data frequently remains proprietary or hidden under “regulatory” pretexts.
Both systems equate secrecy with authority and protect the legitimacy of their monopoly through opacity.
Claims of Serving the Public
Both invoke moral narratives to justify their dominance.
Guilds called themselves servants of craft integrity and urban good.
Medical associations call themselves protectors of patient safety and public health.
Yet in both eras, the practical goal was preservation of professional privilege — not empowerment of the common man or patient.
Co-opting of Regulators
During the late Middle Ages, monarchs legalized guilds in return for taxes or tributes, effectively integrating them into governance.
Today, the medical establishment essentially is the regulator: the FDA, CDC, NIH, and professional associations exchange staff through the revolving door, ensuring that oversight aligns with insider interests.
Today’s Medical guilds have centralized bureaucracies with high operational expenses that are significantly supported by “donations” from pharmaceutical companies and other stakeholders that exert influence surreptitiously and non-transparently promote financial conflicts of interest that align the Medical Guilds with the Pharmaceutical industry and other stakeholders that benefit by influencing Medical Guild policies and practices.
Resistance to Innovation
Guilds:
Slow to adapt to new production techniques because innovation undermines standardized monopoly control.Modern Medicine:
Often suppresses innovative tools and treatments until either large corporations can patent them or regulations can domesticate them. Independent pioneers such as Royal Rife, Linus Pauling, or Abram Hoffer have historically faced institutional ridicule until later vindication.
The medieval Guilds and the modern medical boards and societies share the same soul: an oligopoly draped in moral virtue. Both arose from the belief that unregulated chaos harms people, but both evolved into self-sealing monopolies that suppress creative dissent, alternative innovation, and independent thought.
Reforming medicine today demands what once broke guilds centuries ago — transparency, open access, and freedom to practice without institutional permission. If today’s Medical Guilds will not reform themselves, then governmental organizations, such as Congress, the judiciary, or HHS, will step in. To some extent, this is already happening to the American Academy of Pediatrics. Furthermore, transformational technologies like Artificial Intelligence and “Big Data” analytics will replace the current medical guilds, much as the Industrial Revolution destroyed the power of the Medieval Guilds.
I have two grandsons that are dedicated to the medical community and one is a radiology technician and the other is a nurse. Their choices have been limited due to the time and financial constraints required to achieve a higher level of medical education..
our medical gatekeepers are not doing their job and allowing qualified American born citizens to achieve the best. Consequently, our medical system is importing medical personnel from other countries who do not necessarily understand the culture in America and relate to the patients properly..
My view.
Bring on the great dismantling!
Bust those monopolies.
Make them accountable to patients.