
RSV Vaccine Safety Signals Raise Alarms
Guillain-Barré Syndrome, Preterm Birth, Deaths


Reprinted by permission from Trial Site News
Junchao Li, Affiliated Taizhou People’s Hospital of Nanjing Medical University and colleagues aimed to evaluate post-marketing safety signals for Food and Drug Administration (FDA)-approved respiratory syncytial virus (RSV) vaccines—Arexvy (GSK) and Abrysvo (Pfizer)—by analyzing reports submitted to the Vaccine Adverse Event Reporting System (VAERS) from May 2023 to December 2024.
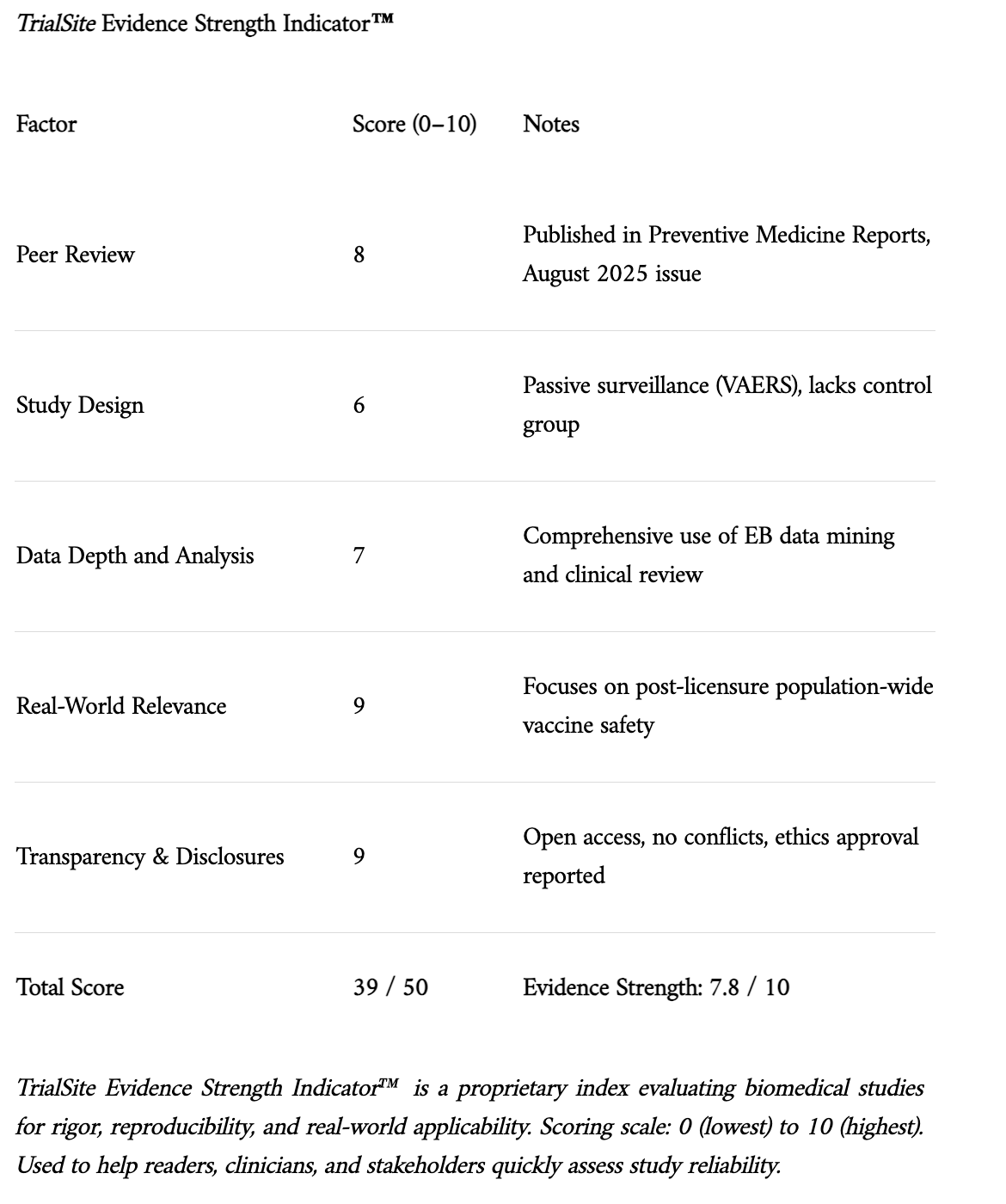
Source: Li, Junchao, Zhiyuan Zhang, and Meixiang Wang. "Post-licensure safety of respiratory syncytial virus vaccines, Vaccine Adverse Event Reporting System, United States, May 2023–December 2024." Preventive Medicine Reports, vol. 56, Aug. 2025, Article 103150.
Study Design and Method
This retrospective surveillance study assessed 6,790 VAERS reports following RSV vaccination. Researchers conducted descriptive analyses, clinical reviews of serious adverse events (AEs), and empirical Bayesian data mining to identify disproportionate reporting signals. Outcomes of interest included Guillain-Barré Syndrome (GBS), preterm delivery, anaphylaxis, and inappropriate administration during pregnancy.
Findings
Among the post-licensure storm clouds trailing the nation’s first RSV vaccines, a few troubling signals flash like distant lightning. The rare, but serious neurological condition Guillain-Barré Syndrome (GBS) surfaced in 81 reports, 59 of which met rigorous diagnostic criteria. Nearly three-quarters of those affected required hospitalization. One case, following administration of Arexvy, ended in death.
Pregnancy-related complications cast a darker shadow still. Among women who received RSV vaccines during pregnancy—especially Pfizer’s Abrysvo—88 reports of preterm birth emerged, some just days after injection. This signal wasn’t subtle; data analysis flagged the frequency of preterm birth with unusually high strength, suggesting the pattern may be more than coincidence. Ten stillbirths and seven cases of preeclampsia further deepen the concern.
The vaccine safety system also recorded 53 deaths, the majority in elderly recipients (median age: 81). The most common culprits: sudden cardiac arrest, respiratory failure, and GBS. While causality cannot be confirmed from VAERS data alone, the timing and clustering of these events deserve serious attention.
Less deadly but still significant were reports of anaphylaxis—14 confirmed cases of severe allergic reaction, some requiring hospitalization—and 44 cases of cellulitis, mostly mild, occurring at or near the injection site.
In a disquieting administrative twist, 367 pregnant individuals were mistakenly given Arexvy—despite its lack of approval for use during pregnancy. While most of these women reported no adverse outcomes, two suffered serious complications, including one case of hypoxic ischemic encephalopathy, a severe condition affecting the infant’s brain due to oxygen deprivation.
Finally, data mining revealed disproportionately high reporting of serious outcomes—GBS, preterm delivery, stillbirth, premature rupture of membranes—especially among younger recipients of Abrysvo. These are not faint statistical whispers but loud signals requiring immediate vigilance and further study.
In sum, while most reports were non-serious and consistent with prior expectations, this post-market snapshot reveals cracks in the veneer of safety for certain populations. The message is not panic—but precision. For the most vulnerable among us—the pregnant, the elderly, and the immunocompromised—ongoing surveillance may mean the difference between prevention and harm
Limitations
As a passive surveillance system, VAERS is subject to underreporting, lack of denominator data, and stimulated reporting biases. The study design does not establish causality. Clinical confirmation was incomplete for several death and GBS reports. Reporting heterogeneity also complicates interpretation across age, vaccine type, and pregnancy status.
Funding and Disclosure
No external funding was received. Authors declared no conflicts of interest. The study was approved by the Ethics Board of Taizhou People’s Hospital and used publicly available, anonymized VAERS data.
Conclusion and Implications
While most adverse events reported after RSV vaccination were non-serious, safety signals for GBS and preterm delivery—especially following Abrysvo in pregnant women—warrant sustained post-market vigilance. The study highlights the risks of off-label administration (e.g., Arexvy during pregnancy) and emphasizes the need for education among healthcare providers to prevent administration errors. Notably, despite emerging safety concerns, the study’s real-world findings remain consistent with Phase III trial signals for GBS and pregnancy-related AEs.
Will repeat, doubt RSV would pose such a threat if the newborn was left alone, no jabs, and let mom' s passive immunity work as it has ever since we climbed down from the trees. And that probably holds true for the host of other jabs given to neonatals. If RSV is as prevalent as advertised mom more than likely is well primed with antibodies to protect her infant.
A key thing not being mentioned in the discussions on the RSV vaccine being added to the schedule is that it is not a "required" vaccine to go to school, whereas most of the other vaccines ACIP approved in the past many parents have no way to opt out of (along with it being a monoclonal antibody rather than a vaccine).