
The Architecture Built While You Weren’t Looking
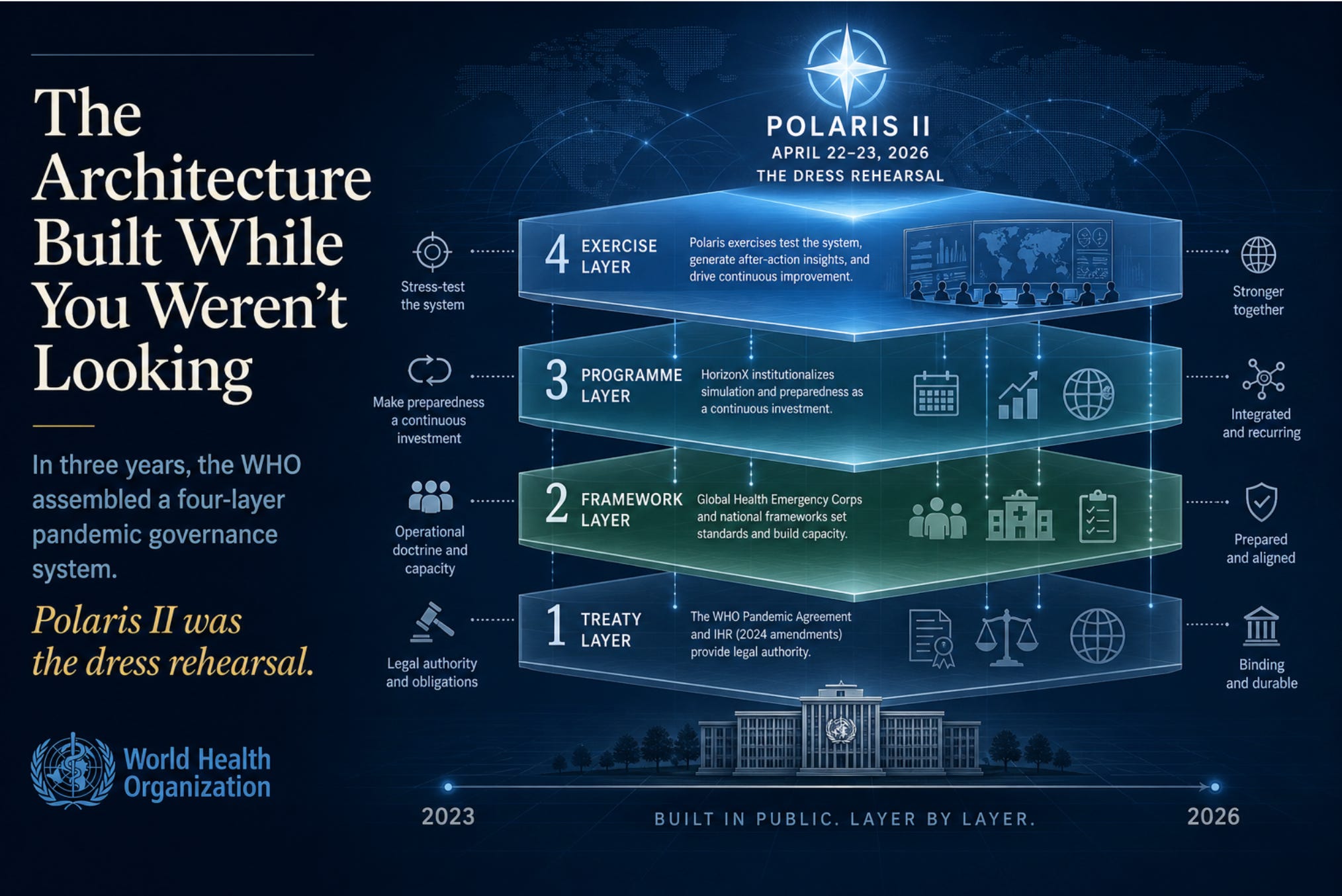
In three years, the WHO has assembled a four-layer pandemic governance system. Polaris II was the dress rehearsal.

While the political class spent the last three years arguing about whether the World Health Organization was secretly trying to take over the world, the WHO did something far more interesting and far more consequential: it built, in plain sight, a complete architecture for managing the next pandemic. And then it ran a dress rehearsal.
The dress rehearsal had a name: Exercise Polaris II. It took place on April 22 and 23, 2026. Twenty-six countries participated, along with 600 health emergency experts and over 25 partner organizations. The scenario was a fictional novel bacterium that had spread across 27 countries and been declared a Public Health Emergency of International Concern.1 Countries activated their emergency coordination structures, mobilized workforces, aligned policies across borders, and (this is worth pausing on) explored AI-enabled tools for workforce planning.2
If you only read the press release, this looks like a tabletop exercise. A drill. A useful one, even, given that the last pandemic killed millions and exposed real coordination failures. Who could object to practice?
But Polaris II is not a standalone event. It is the visible surface of something much larger that has been assembled, piece by piece, since 2023. And once you see the structure, the structure is hard to unsee.
Four Layers, Three Years
What has actually been built is a tightly interlocking, four-layer system that has matured at remarkable speed:
Layer 1: The Treaty Layer. On May 20, 2025, the 78th World Health Assembly adopted the WHO Pandemic Agreement by a vote of 124 in favor, zero against, and 11 abstentions.3 It is only the second legally binding treaty ever negotiated under Article 19 of the WHO Constitution.4 The first was the 2003 Framework Convention on Tobacco Control, and most people have never heard of it because tobacco is unpopular and the treaty was uncontroversial. This one is different. The Pandemic Agreement establishes a Pathogen Access and Benefit Sharing system, a Global Supply Chain and Logistics Network, and a new financial mechanism.5 It enters into force 30 days after 60 ratifications, pending completion of the PABS annex now being negotiated through 2026.6
Sitting alongside the treaty are the 2024 amendments to the International Health Regulations, which came into force in September 2025. Among other changes, they introduced a new “pandemic emergency” alert level, a tier above the existing Public Health Emergency of International Concern designation.7 The IHR has been binding on member states since 2005. The amendments expand its operational reach.
Layer 2: The Framework Layer. The Global Health Emergency Corps was launched at the May 2023 World Health Assembly.8 Its own framework document describes it as “more than a workforce framework; it is a commitment to global solidarity, prioritizing sovereignty and equity.”9 In practice, it is a standing global network of national emergency workforces with mechanisms for surge deployment across borders. It was first activated in October 2024 in response to the mpox outbreak in the Democratic Republic of the Congo.10
In October 2025, the WHO published the National Health Emergency Alert and Response Framework.11 This document tells countries how to structure their domestic emergency response: detection, notification, risk assessment, activation, intervention, review. It embeds the 7-1-7 performance benchmark: seven days to detect an outbreak, one day to notify authorities, seven days to complete early response actions.12 It integrates more than 300 recommendations drawn from COVID-19 reviews into a single national doctrine.13
Layer 3: The Program Layer. HorizonX is the umbrella program that turns simulation exercises from one-off events into a permanent, recurring test regime. It was launched in October 2024 as a multi-year initiative for “multi-sectoral emergency zoonotic disease preparedness.”14 Polaris is just one strand. The WHO ran approximately 50 simulation exercises in 2025 alone.15 The phrase used in WHO’s own materials is telling: preparedness is meant to become “a continuous investment” rather than “a periodic effort.”16
Layer 4: The Exercise Layer. Polaris I in April 2025, with 15+ countries.17 Polaris II in April 2026, with 26.1 Future iterations planned indefinitely under HorizonX. Each exercise stress-tests the layers above it and generates an after-action report that feeds back into framework refinement.18
This is not an accident of bureaucracy. It is a designed system. Each layer reinforces the next. The treaty provides legal authority. The frameworks provide operational doctrine. The program institutionalizes practice. The exercises generate the empirical justification for further build-out.
What the WHO Says About It
The WHO is not secretive about any of this. The Director-General said it plainly after Polaris II concluded: “Exercise Polaris II showed what is possible when we act together. It demonstrated that global cooperation is not optional; it is essential.”19
Read that sentence again. Not optional.
That is not the language of voluntary international coordination among sovereign equals. It is the language of moral obligation backed by institutional architecture. The Director-General is saying (correctly, from his perspective) that the WHO has spent three years building a system in which non-cooperation is no longer a serious option for any country that wants to remain inside the global health order.
A peer-reviewed article in the National Library of Medicine database makes the connection between layers explicit. The Pandemic Agreement, it notes, “reinforces the importance of the GHEC by emphasising that each country should ‘develop, strengthen, and protect a skilled and adequate workforce to prevent, prepare for, and respond to health emergencies, including during pandemics.’” The article continues: “GHEC, with its mandate for rapid response and global health expertise, serves as an operational arm of the Accord. It translates the high-level commitments of the Accord into action.”20
There is no ambiguity here. The framework is the operational arm of the treaty. The exercise tests the framework. The program makes the testing permanent. The treaty makes the whole thing legally durable.
The Sovereignty Question, Honestly Stated
The standard establishment response to concerns about this architecture is to point at specific clauses and say: see, the treaty preserves sovereignty. The text explicitly states it does not authorize the WHO to direct, order, or alter national laws. UK ministers have stated that under no circumstances will the WHO have power to mandate lockdowns.21 WHO spokespeople dismiss the sovereignty concern as misinformation.
These statements are technically accurate. They are also somewhat beside the point.
Sovereignty in the modern administrative state is rarely surrendered by a single dramatic act. It erodes through the accumulation of soft commitments, technical standards, performance benchmarks, peer pressure, funding conditions, and informational dependencies. A country that has signed the Pandemic Agreement, restructured its national emergency workforce per GHEC guidance, adopted the National Alert and Response Framework’s 7-1-7 timelines, integrated its surveillance with the Global Outbreak Alert and Response Network, and committed to participate in HorizonX exercises has not formally surrendered any sovereignty. It has merely made dozens of practical choices that, in aggregate, mean its pandemic response will be functionally indistinguishable from what the WHO would have prescribed.
This is not a conspiracy. It is the normal mechanism by which international technocratic systems operate. The European Union works this way. The IMF works this way. The OECD works this way. What is novel is the speed and scope of the WHO version, and the fact that it is being built specifically around emergency powers, a domain where domestic publics historically grant enormous deference to whoever is identified as the legitimate authority.
When the next pathogen emerges, the question will not be whether national governments retain the legal right to chart their own course. They will. The question will be whether any government, in the heat of an emergency, with its own institutions plugged into WHO frameworks, with its workforce trained on WHO doctrine, with its data flowing through WHO networks, will find it politically possible to deviate. The architecture is being built precisely so the answer is no.
The Funding Question
There is one detail in the WHO’s own Polaris II materials that deserves more attention than it has received. Buried in the WHO Western Pacific feature story on the exercise is a sentence acknowledging that work under the GHEC Initiative is funded by the Gates Foundation and the Institute of Philanthropy.22 This is not a minor footnote. The GHEC is the operational backbone of the entire pandemic response architecture: the standing workforce framework that Polaris exercises, that the Pandemic Agreement reinforces, and that gets activated in real outbreaks. A significant portion of that architecture’s design and implementation has been underwritten by a single private foundation.
Now, you can have two reactions to this. The first reaction, which much of the establishment press takes, is that private philanthropic funding for global health is a longstanding practice, that the Gates Foundation has done genuine good in vaccination and disease eradication, and that pointing this out is the first move in a conspiracy theory. The second reaction is that a global emergency response architecture, with treaty-level legal backing, that operates according to doctrines partly funded and shaped by a single private foundation, raises legitimate questions about democratic accountability that have nothing to do with conspiracy theories.
Both reactions can be true at once. The Gates Foundation’s contributions to global health are real. So is the fact that no electorate anywhere voted for Bill Gates to be a co-architect of the institutional response to the next pandemic. In a constitutional system that takes accountability seriously, “this private actor has good intentions and useful resources” is not a sufficient answer to “who is this person and by what authority does he co-design this.”
What Polaris II Actually Tested
Look closely at the operational details and the implications come into focus.
In Brunei, the Incident Management Team within the national CDC tested airport-linked surveillance and rapid response procedures, then reviewed cross-border traveler monitoring with neighboring countries.23 In Malaysia, the Crisis Preparedness and Response Centre tested activation of the national Incident Management System and coordinated with ASEAN partners.24 Across the exercise, partner organizations contributed to a “global partner mapping survey used in real time during the exercise to simulate the matching of country surge needs with available partner capacity.”25
What is being practiced here is not just medical response. It is integrated, cross-border surveillance of human movement; real-time matching of national needs to international partner capacity; standardized incident management activation across radically different political systems; and the use of AI tools to allocate emergency workforce. These are governance capabilities. They have applications well beyond bacterial outbreaks.
The exercise was framed as a fictional bacterium. The capabilities being rehearsed are agnostic to scenario.
The Honest Defense, and Why It Falls Short
The honest defense of all this goes roughly as follows: COVID-19 killed millions of people and exposed catastrophic failures in international coordination. Surveillance was fragmented, vaccines were hoarded, information flowed unevenly, poor countries got the worst of it, and nobody was in charge. The current architecture is an attempt to fix exactly those failures. Practice exercises are standard. Treaties are how international cooperation works. The 7-1-7 metrics are reasonable performance benchmarks. The whole thing is overdue.
There is real force to this argument, and a serious conservative or libertarian critic should acknowledge it. The COVID response was a disaster. International coordination was bad. The instinct to fix it is not malign.
But the conservative and libertarian objection is not that nothing should be done. It is twofold.
First, the lessons of COVID-19 are contested, and the architecture being built reflects only one set of conclusions. Many serious analysts concluded that the COVID response failed because of too much centralized authority acting on incomplete information, not too little. Lockdowns of unprecedented severity, school closures, vaccine mandates, the suppression of dissent on lab-leak hypotheses, the discrediting of natural immunity, the politicization of early treatment debates; these were failures of centralized authority, not of decentralization. A genuine after-action would weigh both directions of failure. The WHO architecture is being built almost exclusively around the “more coordination” lesson and almost not at all around the “less overreach” lesson.
Second, the speed and scope of the buildout outpace any normal democratic process for evaluating it. Three years from launch of GHEC to a binding treaty, an aligned national framework, an institutionalized exercise program, and two global drills. No national legislature seriously debated the implications. No election anywhere turned on this. The Pandemic Agreement was adopted by consensus at the World Health Assembly with 11 abstentions and no objections, which sounds like overwhelming consensus until you remember that most member state populations have no idea any of this happened.
What to Watch
The PABS annex is being negotiated through 2026 and goes to the 79th World Health Assembly.26 Once adopted, the Pandemic Agreement opens for signature and ratification. After 60 ratifications, it enters into force.6
National parliaments will have a constitutional moment when ratification arrives at their door. In most countries this will receive minimal media attention, and ratification will be treated as a technical formality. In others (and the United States is the most important of these), ratification will be politically contested and may not happen at all. The U.S. position under the current administration on WHO matters generally, and on the Pandemic Agreement specifically, will be one of the more consequential variables in whether this architecture becomes the universal default or a regime that some major countries opt out of.
For now, the structure is built. Polaris II proved it works. HorizonX guarantees it will keep being practiced and refined. The treaty layer is awaiting its final ratifications.
The honest summary is this: between 2023 and 2026, in front of everyone, with full press releases at every stage, the WHO and its partners assembled a four-layer global pandemic governance system more comprehensive and more operationally integrated than anything that has existed before. Whether you think this is overdue progress or quiet overreach depends on what you believe about centralized authority, technocratic governance, and the lessons of the last pandemic.
But the architecture is real. It is not a conspiracy. It is a project. And the project is largely complete.
* * *
If you want to verify any of the facts above, every one of them is sourced from official WHO press releases, the published framework documents, the World Health Assembly resolution, and peer-reviewed analyses. None of it is hidden. That, in a way, is the most striking part.
Bibliography
1. World Health Organization Western Pacific. “Countries showcase global health emergency response and coordination capacities through a WHO-led multi-country simulation.” April 2026. https://www.who.int/westernpacific/newsroom/feature-stories/item/countries-showcase-global-health-emergency-response-and-coordination-capacities-through-a-who-led-multi-country-simulation
2. World Health Organization. “Practicing today for tomorrow’s emergencies – WHO convenes countries and partners to simulate response to major disease outbreak.” 27 April 2026. https://www.who.int/news/item/27-04-2026-practicing-today-for-tomorrow-s-emergencies-who-convenes-countries-and-partners-to-simulate-response-to-major-disease-outbreak
3. UN News. “Nations adopt historic pledge to guard against future pandemics.” 21 May 2025. https://news.un.org/en/story/2025/05/1163451
4. Global Biodefense. “What the WHO Pandemic Agreement and IHR Reforms Mean for the Future of Pandemic Preparedness.” 23 July 2025. https://globalbiodefense.com/2025/07/23/what-the-who-pandemic-agreement-and-ihr-reforms-mean-for-the-future-of-pandemic-preparedness/
5. UN News, “Nations adopt historic pledge to guard against future pandemics,” 21 May 2025.
6. World Health Organization. “WHO Pandemic Agreement.” https://www.who.int/health-topics/who-pandemic-agreement
7. World Health Organization. “Stronger together — milestones that mattered in 2025.” 23 December 2025. https://www.who.int/news-room/spotlight/stronger-together-milestones-that-mattered-in-2025
8. World Health Organization. “Global Health Emergency Corps Framework.” Publication B/78043. https://www.who.int/publications/b/78043
9. International Association of National Public Health Institutes. “WHO Global Health Emergency Corps Framework” (PDF). https://ianphi.org/_includes/documents/sections/tools-resources/ghec-highlights/who-ghec-framework.pdf
10. World Health Organization. “WHO and partners activate Global Health Emergency Corps for the first time in response to mpox outbreak.” 29 October 2024. https://www.who.int/news/item/29-10-2024-who-and-partners-activate-global-health-emergency-corps-for-the-first-time-in-response-to-mpox-outbreak
11. World Health Organization. “National Health Emergency Alert and Response Framework.” Publication 9789240113893. 23 October 2025. https://www.who.int/publications/i/item/9789240113893
12. World Health Organization. “WHO launches new country guidance for health emergency coordination.” 23 October 2025. https://www.who.int/news/item/23-10-2025-who-launches-new-country-guidance-for-health-emergency-coordination
13. WHO, “WHO launches new country guidance for health emergency coordination,” 23 October 2025.
14. World Health Organization. “WHO launches new Horizon X Programme for One Health emergency preparedness.” 13 October 2024. https://www.who.int/news/item/13-10-2024-who-launches-new-horizon-x-programme-for-one-health-emergency-preparedness
15. WHO, “Stronger together — milestones that mattered in 2025,” 23 December 2025.
16. WHO, “Practicing today for tomorrow’s emergencies,” 27 April 2026.
17. World Health Organization. “WHO brings countries together to test collective pandemic response.” 4 April 2025. https://www.who.int/news/item/04-04-2025-who-brings-countries-together-to-test-collective-pandemic-response
18. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
19. WHO, “Practicing today for tomorrow’s emergencies,” 27 April 2026.
20. “Sovereignty, equity, solidarity: progress on the Global Health Emergency Corps.” National Library of Medicine, PMC12374631. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374631/
21. UK House of Commons Library. “What is the proposed WHO Pandemic Preparedness Treaty?” Research Briefing CBP-9550. https://commonslibrary.parliament.uk/research-briefings/cbp-9550/
22. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
23. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
24. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
25. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
Very informative article. Thank you for it.
This appears satanic to me...
It’s always “for the public good.”