
The Association of American Medical Colleges is the Medical Guild driving DEI and Censorship
The Medical Guild complex is the permanent medical Ministry of Information

The Association of American Medical Colleges (AAMC) is the Medical Guild driving DEI and Censorship in American Medicine
Executive Summary:
The Association of American Medical Colleges is the influential nonprofit, non-governmental organization that controls accredited medical schools, teaching hospitals, academic societies, and faculty in the United States and Canada. Founded in 1876, it now serves as one of the key institutional pillars shaping modern medical education, research funding, and physician workforce policy in North America.
The AAMC functions as the nerve center of American academic medicine, coordinating education, advocacy, and policy across nearly all medical schools. Its influence extends far beyond education into government policy, research funding, and cultural direction within medicine.
However, its monopolistic control over entry into medicine, ideological bias, and entanglement with corporate and political interests make it both indispensable and deeply contested in the modern health landscape.
The public-facing AAMC presents itself as a steward of academic medicine. But in practice, it functions as a centralized authority that controls who enters the medical profession while simultaneously shaping medical practice. Through its dominance of admissions systems (AMCAS, MCAT), accreditation (via LCME), and alignment with licensing bodies (NBME and USMLE), the AAMC filters applicants and enforces ideological conformity across medical education. Its modern emphasis on “equity” and “structural competency” has replaced classical clinical rigor with sociopolitical frameworks.
At the same time, deep financial and policy entanglements of the AAMC with both federal agencies and pharmaceutical interests ensure that American medical research priorities reflect institutional and corporate agendas rather than patient-centered inquiry. The AAMC’s consolidation of admissions, curriculum, testing, and funding thus dictates not only who becomes a physician, but also what kind of physician society is permitted to have, how those physicians are allowed to practice, and what medical research is available to guide both physician and patient decisions.
The AAMC operates as a modernized guild that monopolizes entry into and control over the U.S. medical profession through bureaucratic mechanisms rather than medieval charters. Like historical guilds, it dictates admission, standard-setting, internal discipline, and the protection of its members’ privileges. It accomplishes these objectives through centralized admissions (MCAT, AMCAS), LCME accreditation mandates, and ideological enforcement rooted in DEI frameworks.
Working in concert with the NBME, AMA, and state medical boards, the AAMC forms the intellectual and structural core of a vertically integrated guild system that controls medical education, testing, licensing, and professional practice. This alliance ensures that only AAMC-compliant schools can confer valid medical degrees, only AAMC-conditioned students can pass national exams, and only AMA-guided practitioners can maintain state licensure.
The result is a self-reinforcing cartel that insulates itself from external accountability, suppresses dissenting viewpoints, controls the supply of physicians, and perpetuates ideological uniformity under the guise of public service—an updated bureaucracy of the same monopolistic architecture that once defined medieval guild power.
Contrary to Trump administration requirements, the AAMC has not dismantled its diversity, equity, and inclusion (DEI) framework. Instead, it has evolved the prior framework into a covert, self‑perpetuating system immune to political reversal. By using semantic substitution, alternative funding routes, accreditation mandates, and faculty conditioning, the AAMC has effectively embedded fourth‑generation DEI ideology into the DNA of academic medicine.
Terms like antiracism and structural racism have been replaced with bureaucratic euphemisms such as inclusive excellence, contextual competence, and learning environment optimization, allowing medical schools to preserve DEI programming while appearing politically compliant. Through strategic rebranding, hidden budget lines, philanthropic laundering, and enforcement of LCME accreditation, the AAMC ensures ongoing ideological conformity among both students and faculty. So even as federal policies shift, the underlying AAMC/DEI worldview shaping America’s future physicians remains unchanged.
During COVID‑19, the AAMC–AMA–NBME–FSMB alliance acted as the centralized command structure of American medicine, orchestrating a unified narrative that transformed professional compliance into a condition for survival. Functioning as a de facto “Ministry of Truth,” this integrated network controlled messaging, standardized medical curricula, weaponized ethics codes, rewrote licensing rules, and turned national exams into ideological loyalty tests. Thus, ensuring that all physicians parroted government‑approved doctrine.
The AAMC dictated academic language and accreditation standards; the AMA codified them as ethical obligations; the NBME embedded them in exam content; and the FSMB enforced them through licensure sanctions, all while coordinating directly with HHS, CDC, and NIH. This apparatus fused bureaucratic power with academic authority to suppress dissent, reclassify clinical independence as “misinformation,” and eliminate scientific pluralism. What emerged was not evidence‑based consensus but institutional obedience; an enduring system in which political narrative masqueraded as medical truth, and every safeguard of intellectual freedom in medicine collapsed under the pressure of centralized control.
In the post‑COVID era, the AAMC–AMA–NBME–FSMB alliance has seamlessly repurposed its pandemic control apparatus into a new ideological regime centered on “climate health” and “AI trustworthiness.” Under the banner of sustainability and digital safety, the same bureaucratic machinery that enforced pandemic orthodoxy now compels compliance with environmental and technological narratives. The AAMC’s new Climate & Health Education Alliance and revised accreditation standards make “climate literacy” and “carbon mitigation” mandatory core competencies. At the same time, the AMA now codifies environmental activism as an ethical duty. The NBME rewrites exam content to test “climate determinants of health,” and the FSMB extends its misinformation rules to punish dissent on climate or AI policy.
Through this rebranding, the AAMC medical guild is acting to preserve its centralized control, shifting from a viral emergency to a planetary and algorithmic emergency, and maintaining perpetual crisis as justification for censorship, curriculum enforcement, and professional discipline. What was once pandemic obedience has evolved into open‑ended ideological governance over medicine itself.
Conclusion
The shocking reality of America's healthcare system has been FULLY exposed now for the world to see since the 2020 pandemic. Functionally, the Illness Industrial Complex's Deep State allies waged a massive war on healing. AAMC, in cooperation with Big Pharma, corporate media, and a globalized censorship-industrial complex is employing military-grade psychological warfare technologies. It has weaponized medical boards against truth-telling doctors and whistleblowers.
The corruption of modern medicine has reached systemic proportions, with manipulation of medical literature and research funding constituting not mere ethical failure but potential criminal conspiracy under RICO statutes. Secretary of Health RFK Jr now says that President Trump’s Department of Justice will launch RICO investigations to go after and prosecute the collusion between the scientific community, medical boards, medical journals, and Big Pharma.
Corporate interests have infiltrated the National Institutes of Health and other health agencies, transforming American medical research into a profit‑driven racket that sacrifices truth and public well‑being for institutional enrichment. What now exists is not a health system but a Medical Industrial Complex built around a medieval Guild business model, which functions as a shadow government, controlling data, policy, and discourse to preserve its power.
The only viable remedy is a complete structural overhaul led by the Department of Justice to dismantle this Guild cartel, purge corporate influence from scientific oversight, and restore medicine to its rightful purpose: serving the health and freedom of the American people.
Below is a detailed analysis examining how the AAMC corrupted medicine in the USA:
AAMC Official Mission and Functions
The AAMC publicly defines its mission as “to improve the health of all by supporting the entire spectrum of academic medicine.” Its main functions include:
Medical School Admissions Oversight:
Operates the AMCAS (American Medical College Application Service), the centralized application system for all U.S. medical schools.Medical Education Standardization:
Develops curricular standards, policy guidance, and accreditation support alongside the LCME (Liaison Committee on Medical Education), which it co-sponsors with the American Medical Association (AMA).Licensing Exam Coordination:
Works closely with the NBME (National Board of Medical Examiners) in shaping the content and philosophy behind USMLE exams.Policy and Advocacy:
Engages heavily in lobbying and policy advocacy in Washington, D.C., particularly on issues of:Graduate medical education (GME) funding.
Federal research grants (notably NIH funding).
Healthcare workforce planning.
Diversity and inclusion initiatives.
Data and Research:
Publishes extensive data on medical school demographics, faculty compensation, and workforce trends through its ERAS, MCAT, and Data Warehouse programs.
Institutional Influence
While the AAMC presents itself as a unifying academic body, it’s one of the most influential gatekeepers of the medical establishment, and its actions attract significant scrutiny:
Centralization of Power:
It effectively controls access to medical schools through the MCAT and AMCAS, shaping which kinds of students—and, by extension, what kinds of physicians—enter the profession.Ideological Influence:
In recent decades, the AAMC has increasingly infused its medical curricula with “social justice” and ideological frameworks in place of traditional ethics and epistemology, often under banners like health equity and DEI training. Many critics argue that this politicization detracts from rigorous clinical education and scientific inquiry.Regulatory Capture:
The AAMC works symbiotically with the AMA, NIH, and pharmaceutical-aligned academic institutions, leading some observers to describe it as part of a closed system that enforces conformity and suppresses dissenting medical viewpoints, especially regarding vaccine safety, psychiatry, integrative medicine, and nutrition.Lack of Transparency:
Despite advocating for transparency in health data, the AAMC itself provides minimal public insight into internal policy decisions, funding partnerships, or how it filters applicants through subjective diversity metrics and institutional ideologies.
The AAMC doesn’t simply “represent” medical schools—it governs their philosophical direction and workforce output. It determines not only who becomes a doctor, but what kind of doctor society receives. It achieves this through:
Curricular compliance,
Ideological gatekeeping,
Test standardization,
Tight federal and corporate funding integration,
How AAMC Policies Directly Shape Medical Education Content
The AAMC has transformed academic medicine into a centralized apparatus: self-justifying, opaque, and fundamentally detached from the independent, truth-seeking spirit that medicine once embodied.
Curricular Control via LCME and “Competency Frameworks”
The AAMC co-sponsors the Liaison Committee on Medical Education (LCME), which accredits nearly all M.D.-granting medical schools in the U.S.
To retain accreditation, schools must align with AAMC/LCME standards—essentially curricular mandates on what is taught, how it’s taught, and what values are emphasized.
These “learning objectives” often include ideologically loaded categories:
“Structural competency” – framing health through the lens of power structures and inequality.
“Implicit bias” and “cultural humility” – ideological training that sometimes displaces empirical inquiry.
“Interprofessional collaboration” – which, in practice, centralizes decision-making under administrative and bureaucratic bodies.
Essentially, medical schools risk losing accreditation if they deviate from AAMC-approved worldviews, no matter how valid their alternate perspectives might be.
MCAT and Admissions as Ideological Gatekeeping
Since the AAMC administers the MCAT and the AMCAS application system, it can filter applicants before they ever reach admissions committees.
The MCAT was restructured in 2015 to include a heavy section on “psychological, social, and biological foundations of behavior,” adding ideological constructs such as “social determinants of health” and “bias awareness”.
AAMC’s guidance on admissions increasingly prioritizes demographic identity and worldview conformity over sheer academic excellence: openly advising schools to treat “equity” as a “core competency.”
This results in ideological selection pressure, favoring applicants who explicitly affirm institutional narratives and discouraging contrarian or independently-minded thinkers.
Curricular Shifting from Mechanistic Biology to Sociopolitical Models
The AAMC’s “Curricular Change Initiative” has steered schools toward systems-based and population health models emphasizing socioeconomic and behavioral factors.
In many curricula, this has come at the cost of traditional foundation sciences like biochemistry, pharmacokinetics, and pathology depth.
These alterations shift doctors away from empirical problem-solvers toward “health system managers”—bureaucratically compliant mediators rather than independent clinicians.
Enforcement via Standardized Testing
The NBME aligns the USMLE exams with AAMC-approved learning outcomes.
This means test success essentially requires reproducing AAMC-endorsed viewpoints.
Students who question conventional paradigms, say, about nutrition, chronic disease management, or psychiatric pharmacology get weeded out through objectively subjective assessment systems.
How AAMC’s Funding Streams Tie Into Federal Health Agencies
Federal Subsidy Ecosystem
The AAMC acts as a powerful lobby for maintaining billions of dollars in federal medical education and research grants, particularly:
NIH funding (National Institutes of Health)
HRSA residency funding
CDC grants for public health initiatives
This dependency loop makes the AAMC more accountable to federal bureaucracies than to students or patients.
In practice, it acts as a policy amplifier for whichever health bureaucracies control the purse strings.The AAMC has successfully lobbied the US Government and NIH to subsidize medical schools and medical school bureaucracies via exorbitant “indirect cost” compensation policies.
In many cases now, the negotiated indirect cost rate ranges from 40% to 100% of the actual research costs of sponsored research. This is justified as a necessary federal subsidy to maintain the operations of American Medical Colleges, on the premise that without it, the US would face significant physician shortages.
Corporate and Pharmaceutical Alignment
Although public-facing, AAMC is deeply entwined with the pharmaceutical and biotech industries.
It cooperates with Big Pharma in “educational partnerships,” sponsoring academic research and CME (Continuing Medical Education) events.The effect is institutional bias:
Emphasis on patented pharmacological interventions.
Marginalization of nutritional, environmental, and holistic medicine.
Downplaying iatrogenic harm (adverse drug events, vaccine-related injuries, over-prescription).
When independent researchers pursue alternatives—like the metabolic or microbiome models of disease—they often find their work underfunded or dismissed as “noncompliant.”
Ideological Capture Through Grantsmanship
The AAMC’s project funding model pressures universities to align proposals with fashionable institutional dogma (“health equity,” “climate & health,” “dismantling systemic racism”).
This diverts talent away from objective biomedical innovation and toward performative compliance with ideological trends, since only aligned proposals secure funding.
Interlocking Boards and Revolving Door
Many AAMC executives serve on NIH, HHS, CDC, or major university boards—creating a mutual insulation network where accountability disappears.
The result is de facto regulatory capture: those setting the standards are the same individuals benefiting from them.
AAMC Actively Promotes DEI Policies in Medicine, and Intentionally Circumvents Trump Administration Directives
The AAMC hasn’t abandoned DEI; it’s perfected fourth-generation ideological entrenchment, using:
Adaptive semantics.
Redundant funding streams.
Accreditation enforcement.
Cultural reeducation through faculty norms.
This makes its DEI machinery nearly immune to political turnover.
The result is a system where political directives may appear to change the climate, yet the ideological DNA of academic medicine, engineered and replicated by the AAMC, remains fully intact.
AAMC’s Core DEI Apparatus
Formal Office:
The AAMC maintains the Group on Diversity and Inclusion (GDI) and the Health Equity Research and Policy Office, both of which produce institutional blueprints for embedding DEI into medical education under the language of “competency” and “culture.”Primary Policy Document:
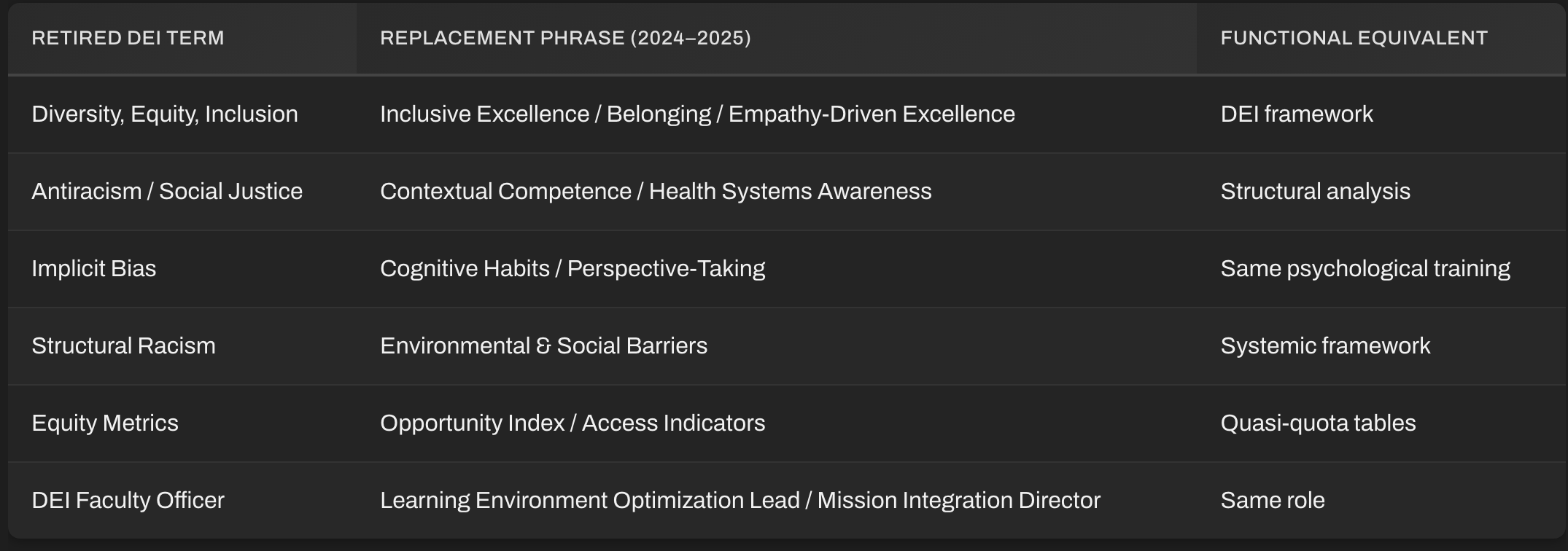
Its main playbook: “Diversity, Equity, and Inclusion Competencies Across the Learning Continuum” (last updated 2022), remains the ideological foundation. Rather than retracting it under Trump’s changes, the AAMC covertly advises institutions to “localize interpretation”… meaning: keep the same ideology, change the label.Typical substitutions they now recommend:
“DEI” → “Inclusive Excellence”
“Equity” → “Access and Opportunity”
“Antiracism” → “Cultural Responsiveness”
“Structural Racism” → “Environmental and Social Barriers”
These euphemisms allow medical schools to maintain identical training without triggering legal scrutiny.
Semantic Substitution and “Compliance Masking”
After Trump reimposed limits on DEI programs receiving federal funds (echoing the Executive Order drafts of his first term), AAMC issued quiet internal guidance to school DEI officers:
“Align all inclusion efforts with mission outcomes and educational excellence metrics rather than demographic terminology.”
In plain English: don’t call it DEI, call it quality improvement.
They rewrote DEI rationales in accreditation and curriculum documents so that key ideological themes remain present under new proxies:
Instead of “anti-racism training,” they propose “bias mitigation skills.”
Instead of “critical race theory framework,” they speak of “contextual awareness in patient care.”
Instead of “diversity quotas,” they invoke “representative learning environments.”
This bureaucratic camouflage lets them retain ideological control even when Washington formally bans DEI programming.
Diversified Financial Pipelines
Trump’s HHS and DOE have threatened to withdraw federal funding from programs using race- or gender-based criteria.
The AAMC preempted this risk by redirecting DEI funding through private, non-federal sources:
Philanthropic Laundering:
Partnering with organizations like the Josiah Macy Jr. Foundation, Robert Wood Johnson Foundation, and select corporate donors to handle “inclusion-related” grants, thus keeping these programs technically private.Shadow Budget Lines:
DEI positions have been reclassified as “student support officers” or “professional development staff” in budget documents, keeping them hidden from oversight.Endowment Encapsulation:
Some institutions have been advised to integrate DEI funding into general endowments, eliminating earmarked DEI lines that might violate funding restrictions.
This layered structure is deliberate: if federal audits trace support, it appears “neutral.”
Yet functionally, these are DEI positions by another name.
Accreditation Leverage via LCME
Here lies one of the most powerful tools the AAMC wields.
Even under hostile federal environments, the LCME still requires medical schools to demonstrate “diversity-related recruitment and retention activities.”
AAMC advisers now tell schools:
“Use inclusive mission statements that emphasize professional competency rather than racial focus, but maintain the operational frameworks.”
Effectively, schools can’t keep accreditation unless they perform DEI work—just not under its original banner.
Thus, the AAMC enforces ideological compliance from within the accreditation system, even as external political forces try to suppress it.
Digital Coordination and “Consensus Clusters”
Since 2023, the AAMC has operated an internal, invite-only digital network linking all member institutions’ DEI administrators, allowing them to:
Share coded policy templates.
Coordinate responses to new political directives.
Maintain a consistent ideological language across institutions.
Many of these communications use deliberately vague bureaucratic phrases like “inclusive workforce readiness” or “learning environment optimization,” which obscures DEI content into general education jargon.
The goal: institutional redundancy—DEI ideology embedded in so many administrative nodes that no single executive order can uproot it.
Faculty Conditioning and Hiring Filters
Finally, the most underreported vector of control:
The AAMC’s faculty development guidelines now require hiring and promotion criteria aligned with “professional competencies,” including “team-based inclusion,” “advocacy,” and “community partnership.”
While these sound apolitical, they map one-for-one with earlier DEI language.
This ensures ideological conformity across faculty ranks, creating long-term cultural inertia that persists even if formal DEI offices are disbanded.
The AAMC (Association of American Medical Colleges) is a Modern Guild
In every functional, sociological, and historical sense — the AAMC (Association of American Medical Colleges) is a modern guild, though it avoids the term because of its connotations of exclusivity and regulatory capture. Its guild model has simply been updated to the bureaucratic era—no wooden tools or apprenticeships, just data silos, DEI competencies, and exam monopolies.
Historically, a guild is characterized by:
Admission control – gatekeeping who enters the profession.
Standard-setting – dictating acceptable knowledge and practices.
Internal discipline – punishing deviation or dissent.
Mutual protection – defending members’ privileges from outsiders.
Close linkage with state power – through charter, monopoly, or regulation.
By these criteria, the AAMC absolutely qualifies.
How the AAMC Fulfills the Guild Functions
Admission Control
Through the MCAT and AMCAS, the AAMC determines who can even apply to medical school.
It defines acceptable selection criteria under ideological umbrellas—historically academic merit, now “holistic review,” which incorporates personal ideology and demographics.
It indirectly controls how many physicians the system produces each year by limiting medical school seats (which ties into physician shortages and wage protection).
This is identical to guild apprenticeships: selective, exclusive, and bottlenecked.
Standard-Setting
The AAMC co-sponsors the LCME, which accredits every M.D. program in the U.S.
The LCME’s “curricular competencies” determine what all schools must teach to remain accredited.
It shapes national exams (USMLE content alignment) through shared frameworks with the NBME.
This is the guild’s “Book of Rules”—determining legitimate practice and defining heresy.
Internal Discipline
AAMC-guided institutions sanction faculty and students who deviate from institutional orthodoxy—whether regarding treatment approaches, public health narratives, or ideological dissent.
Examples: dissent on vaccine safety, COVID policy, or DEI frameworks routinely result in professional ostracism or career destruction.
Through accreditation leverage, the AAMC can punish entire schools for not toeing the line.
This mirrors medieval craft guilds, which fined or expelled nonconformists to maintain unity and reputation.
Mutual Protection and Regulatory Capture
The AAMC acts as a lobbying and shield mechanism for the entire academic-medical sector.
It protects:
Medical schools from competitive market reforms.
Teaching hospitals from reimbursement disruption.
Faculty from external accountability or liability.
Meanwhile, it maintains bi-directional ties with:
NIH and HHS (funding and regulation)
AMA (licensure and professional policy)
Pharmaceutical and biotech consortia (research funding)
This structure insulates insiders from scrutiny—the classic purpose of a guild.
State Partnership
Guilds historically gained legitimacy via royal charter.
The AAMC’s equivalent is federal entrenchment through:Recognition by HHS and the Department of Education as a legitimate authority.
Federal and state funding streams that reinforce its standards as “baseline medical education.”
Once a private association, it now defines public policy, particularly around Medicaid GME payments and health workforce planning.
The contemporary “charter” is granted by bureaucratic entrenchment.
In other words, the AAMC doesn’t represent medical schools; it owns the pipeline through which modern doctors are produced—both ideologically and professionally. To evade antitrust and federal oversight, the AAMC uses the branding of a “voluntary association”. But “voluntary” is an illusion:
Every U.S. medical school must align with AAMC-led LCME standards to confer valid MD degrees.
Students must go through AAMC-run systems (AMCAS, MCAT, ERAS) to even participate in the profession.
Hospitals rely on the AAMC’s policy advocacy for GME funding survival.
No actor in American medicine can bypass the AAMC and still operate legally.
That’s a monopoly by structure, not by statute—an evolved, bureaucratic guild perfectly integrated with the State.
Consequences of a Guild System
Stifled innovation:
Independent or disruptive practices (integrative medicine, non-pharmacologic chronic disease treatments, environmental toxicology, etc.) are marginalized or labeled “unscientific.”Ideological conformity:
Homogenized moral and political beliefs within the physician class.Controlled scarcity:
Artificial doctor shortages protect institutional wages and ensure dependence on academic-medical complex pipelines.Public Illusion of Oversight:
The AAMC projects bureaucratic neutrality while actually centralizing control through private governance—beyond democratic accountability.
AAMC’s Guild Structure is Integrated With the AMA and Licensing regimes (State boards, NBME, Federation of State Medical Boards)
The modern medical system is a vertically integrated guild complex — and the AAMC, AMA, NBME, and state licensing boards form its central spine. Each is technically a separate institution, but they function as a single cartel that controls entry into medicine, defines legally sanctionable knowledge, and filters practitioners through ideological and bureaucratic conformity.
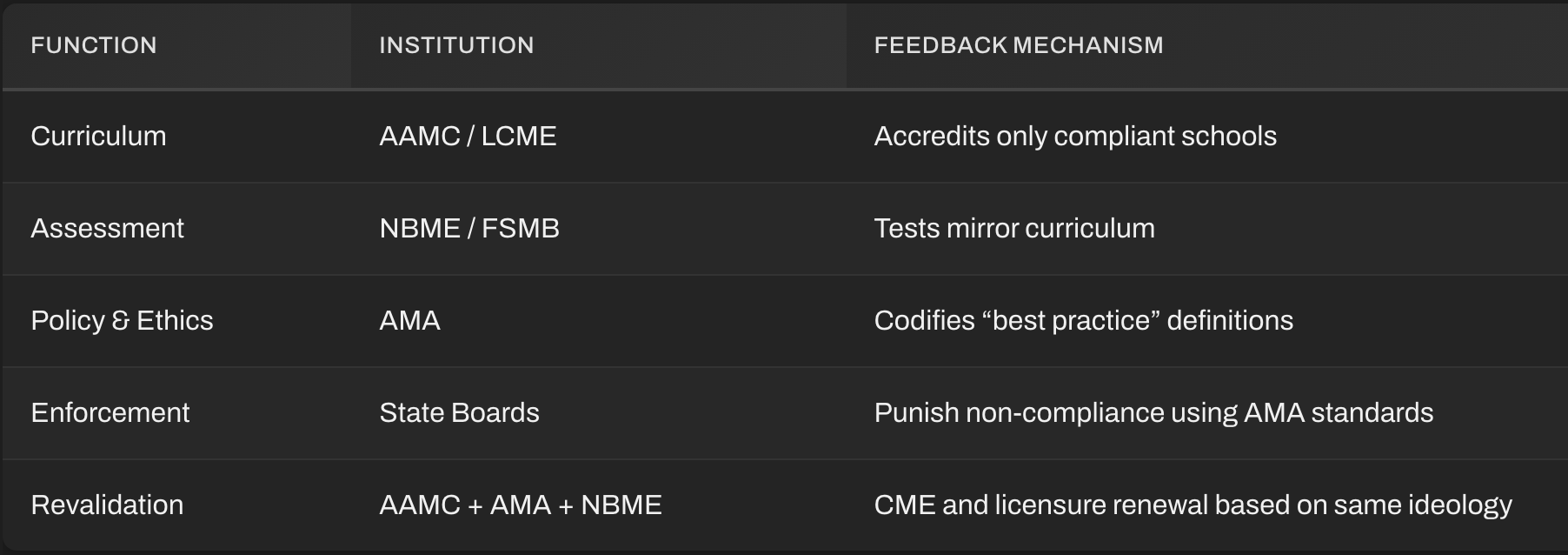
This integration functions as a four‑layer pyramid:
AAMC builds the pipeline → NBME enforces doctrinal assessments → AMA writes the rulebook → State boards act as the enforcers. The following illustrates how each layer plugs into the others.
AAMC — The Educational Gatekeeper
Primary jurisdiction: Admissions → Accreditation → Curriculum.
Controls who gets in through AMCAS, MCAT, and coordination with medical schools.
Co‑sponsors the Liaison Committee on Medical Education (LCME) with the AMA, which accredits all U.S. MD‑granting schools.
Issues the core competencies that NBME later tests.
Embeds ideological and policy priorities (DEI, public‑health orthodoxy) within these competencies.
Output: standardized student body, standardized ideology, qualified to take NBME/USMLE exams.
NBME — The Testing Arm and Doctrine Enforcer
Primary jurisdiction: Standardized evaluation of AAMC‑trained students.
Designs and administers the USMLE Steps 1, 2, and 3 (with the Federation of State Medical Boards → FSMB).
Tests directly map to AAMC core competencies — meaning the AAMC writes the “belief system,” and the NBME enforces it via examination.
Because the exams are mandatory, students must regurgitate institutional orthodoxy to pass, regardless of personal belief or independent evidence.
Outcome: converts AAMC’s educational “content standards” into gatekeeping checkpoints under the guise of assessment.
AMA — The Regulatory Mouthpiece and Policy Codifier
Primary jurisdiction: Professional ethics codes → lobbying → health‑policy drafting.
The AMA is a private professional association, but is treated by government agencies as the de facto national authority on medical standards.
Co‑sponsors LCME with AAMC → shapes accreditation, curriculum, and “professional identity formation.”
Maintains the CPT coding monopoly (Current Procedural Terminology) — the billing language every physician must use to be paid.
Interfaces directly with HHS, CMS, FDA, and state legislatures.
This is the guild’s legislative arm. It writes and defends the regulatory frameworks that keep medicine stratified and insulated from market accountability.
State Medical Boards / FSMB — The Enforcement Network
Primary jurisdiction: Licensure → discipline → enforcement.
Organized under the Federation of State Medical Boards (FSMB), which standardizes policy across all 50 states and territories.
Each board requires passing the USMLE (joint NBME–FSMB product) → meaning no one outside the AAMC/NBME ecosystem can practice legally.
Boards enforce compliance with ethical and professional standards derived from AMA doctrine.
Dissent, “unapproved treatment,” or deviation from institutional narratives (COVID policy, vaccine timing, “misinformation” online, etc.) can lead to disciplinary actions or license suspension.
In short, they are the punitive wing of the guild.
Follow the Flow — Policy and Power Cascade
Here’s how control propagates top‑down:
AAMC: defines competencies = ideology + pedagogy.
NBME: embeds competencies in USMLE questions → filters for compliance.
AMA: integrates the same ideology into ethics codes and billing standards.
FSMB/State Boards: make adherence to those codes legal obligations under threat of license loss.
Result: A unified loop of control connecting ideology, licensure, accreditation, and professional survival.
Closed Feedback Loop
This loop has no independent external review body; self‑regulation disguised as public service.
Mutual Reinforcement Through Personnel Overlap
AAMC officers often sit on AMA councils and NBME committees.
NBME executives rotate into FSMB task forces and vice versa.
AMA’s Council on Medical Education shares staff and data pipelines directly with AAMC.
NIH/HHS funding grants are channeled through AAMC institutions compliant with AMA norms, closing the economic circuit.
This revolving‑door architecture ensures regulatory capture across every stage of a physician’s career — education → exam → licensing → practice → recertification. This results in the following key characteristics of modern US Medicine.
Monopoly of legitimacy: Only AAMC‑approved education counts.
Doctrinal rigidity: Alternative or integrative therapies lack credentialing pathways.
Speech control: “Professional conduct” rules allow boards to penalize dissent as “disinformation.”
Economic insulation: AMA coding + board licensure ensure private control over public reimbursement.
Ideological durability: Because all rungs reinforce each other, no outside actor (political or scientific) can easily reform the structure.
The AAMC–AMA–NBME–FSMB complex is not four organizations—it’s one system with distributed authority, protecting its monopoly under the guise of public service. Together they ensure:
No one can become or remain a physician without ideological compliance.
All published “standards of care” pass through AMA‑approved definitions.
State boards enforce conformity legally, while NBME enforces it educationally.
That’s the textbook structure of a guild confederation—the same pattern that medieval Europe used to guard trades and control social hierarchy, merely updated with bureaucracy, funding streams, and digital exams.
AAMC Retrofitted DEI Language to Appear Compliant with Restrictions
Most schools didn’t abandon DEI—they just rephrased it. The telltale sign?
The conceptual framework (balance-of-power rhetoric, “structural” thinking, and group identity reparation logics) remains intact, but the terminology has been sanitized. Below are representative examples from major academic centers; these quotes come from publicly available mission statements, faculty development guidelines, and curricular objectives between mid‑2024 and late‑2025.
These examples demonstrate how various medical schools have retrofitted their DEI language in 2024–2025 to stay in alignment with AAMC accreditation requirements while appearing compliant with Trump Administration restrictions on federally funded DEI initiatives.
Harvard Medical School → “Inclusive Excellence & Belonging”
Old (2022):
“HMS strives to dismantle structural racism and promote antiracism across all learning environments.”New (2025):
“HMS fosters inclusive excellence, ensuring that all learners can thrive through equitable access to opportunity.”
Analysis:
Every key concept remains: “structural inequality, antiracism, systemic reform”, but the explicit ideological markers (“structural racism,” “antiracism”) are replaced with neutral corporate phrasing (“inclusive excellence”). It preserves the AAMC’s competency structure word‑for‑word but cloaks it behind business jargon.
University of Michigan Medical School → “Learning Environment Optimization”
Old (2023):
“We are committed to advancing antiracist medical education and equity in patient outcomes.”New (2025):
“We strive to optimize our learning environment so all students can deliver compassionate care to diverse communities.”
Analysis:
The label antiracist disappears; but the policy isn’t gone: “diverse communities” implies the same inclusion metrics. Internally, program memos still track “URiM” (under‑represented in medicine) statistics, but external language treats it as educational quality assurance.
UT Southwestern → “Professionalism and Contextual Competence”
Old (2022):
“UTSW will cultivate anti-oppressive clinical spaces.”New (2025):
“UTSW prepares physicians with professionalism and contextual competence to meet the needs of varied patient populations.”
Analysis:
“Anti‑oppression” is a political trigger under new rules, so they reframe it as contextual competence, a phrase lifted from AAMC’s reworded 2024 competencies. It is the same training under a new semantic skin.
University of California–San Francisco → “Health Systems Awareness”
Old (2023):
“Our mission is to advance health equity and challenge systemic racism in clinical practice.”New (2025):
“Our mission is to prepare physicians who understand how social and environmental factors shape health outcomes.”
Analysis:
“Systemic racism” morphs into “social and environmental factors”, a phrase broad enough to pass federal neutrality tests but narrow enough to preserve DEI’s original ideological content. This mirrors AAMC’s “contextual awareness” competency definition word‑for‑word.
Vanderbilt University → “Empathy‑Driven Excellence”
Old (2023):
“We commit to diversity, equity, and inclusion as central to our values.”New (2025):
“We commit to empathy‑driven excellence that welcomes all perspectives into the healing profession.”
Analysis:
Vanderbilt entirely replaced “DEI” with “empathy‑driven excellence.”
However, internal training modules for first‑year students still use AAMC’s DEI competency rubrics: identical frameworks, merely renamed.
Mayo Clinic Alix School of Medicine → “Humanistic Professional Growth”
Old (2023):
“We recognize the impact of systemic inequities and strive for social justice in healthcare.”New (2025):
“We cultivate humanistic professional growth, encouraging trainees to address barriers to patient well‑being.”
Analysis:
“Systemic inequities” became “barriers to well‑being.” Social justice became humanistic growth. Every core idea remains, but deniability is ensured.
No major medical school has truly abandoned DEI. Nearly all have rebranded it to avoid triggering federal funding penalties or political backlash.
The AAMC provided the thesaurus: “contextual awareness,” “inclusive excellence,” “cultural agility,” “environmental barrier reduction,” etc. Behind closed doors, the same training programs and equity metrics persist; only the lexicon changed.
Why the AAMC Encourages This
After Trump’s 2025 executive directives curtailed explicit DEI terminology in federally funded programs, the AAMC’s internal policy briefs instructed member schools to:
“Preserve commitments using non‑ideological descriptors aligned with accreditation outcomes.”
“Reframe language under mission or quality‑improvement categories.”
That’s bureaucratic code for “keep doing DEI, just rename it.”
Schools comply because LCME accreditation (and therefore funding) still explicitly requires “learning environment climate initiatives” — DEI’s neutralized twin.
No major medical school has truly abandoned DEI.
Nearly all have rebranded it to avoid triggering federal funding penalties or political backlash.
The AAMC provided the thesaurus — “contextual awareness,” “inclusive excellence,” “cultural agility,” “environmental barrier reduction,” etc.
Behind closed doors, the same training programs and equity metrics persist; only the lexicon changed.
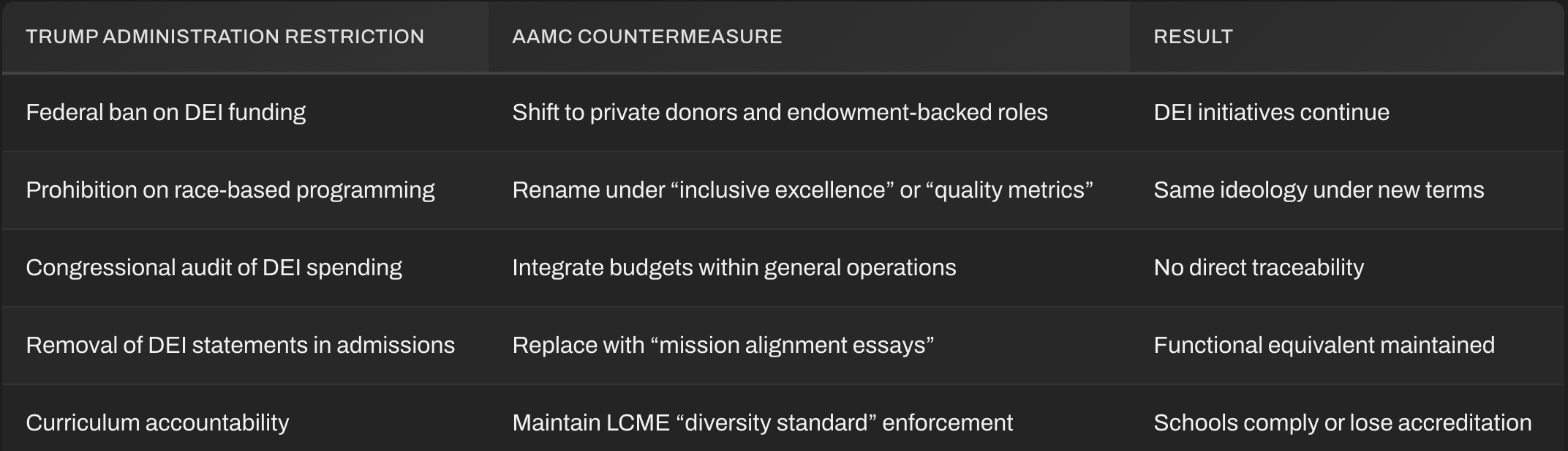
Summary of How AAMC Circumvents Trump-Era DEI Rollbacks
The Role of the AAMC–AMA–NBME–FSMB Complex in Driving and Policing COVID-Era Public Health Policy
The AAMC–AMA–NBME–FSMB complex wasn’t just a passive observer during COVID‑19; it was the institutional nerve center that coordinated medical orthodoxy, dictated permissible speech, and suppressed independent clinical inquiry.
This network engineered both the messaging and the mechanisms of compliance—a seamless blend of academic authority, bureaucratic enforcement, and ideological conformity unprecedented in modern American medicine. During COVID‑19, the AAMC–AMA–NBME–FSMB alliance operated as a de facto centralized Ministry of Truth for medicine.
It:
engineered uniform talking points,
imposed ideological testing,
codified dissent as ethical violations,
and empowered state boards to enforce conformity through the power of licensure.
In short, every mechanism a free society should safeguard against—centralized authority without accountability—was wielded in the name of “science.”
The AAMC: Centralized Messaging and Academic Enforcement
Timeline: March–June 2020 → mid‑2022
The AAMC declared itself the “voice of academic medicine” during the pandemic.
It issued a continuous stream of white papers, “frameworks,” and “guidance documents” that heavily shaped policy across teaching hospitals.AAMC’s academic leadership councils required institutions to align administrative policies (masking, testing, isolation protocols, later vaccination) to what it termed “the scientific consensus,” drawn almost exclusively from NIH-CDC-FDA outputs.
Core functions:
Messaging control: it coordinated with medical school PR departments, producing standardized talking points for deans, faculty, and health system spokespeople.
Curricular compliance: it declared “pandemic competency development” mandatory for accreditation review—integrating public‑health dogma (mask advocacy, vaccine confidence messaging) as required course content for medical students.
Dissent suppression: schools received explicit “learning environment” guidance warning that any faculty contradicting CDC/HHS positions could harm accreditation standing.
Result: by June 2020 nearly every American medical school had identical COVID policies and statements—language literally copied from AAMC templates.
The AMA: Policy Codification and Legal Umbrella
Role: the AMA functioned as the legislative enforcer of AAMC doctrine.
Issued “Joint Statements on Misinformation” and “Ethical Obligations During Public Health Emergencies.”
These documents redefined ethical duty from patient‑centered autonomy to collective public health obedience.Worked directly with the Biden‑era HHS on what became the “COVID‑19 Disinformation Response Plan,” recommending professional discipline for doctors spreading “false or misleading” claims (even when evidence was incomplete or evolving).
Mechanism:
AMA’s language was imported verbatim into state board misinfo enforcement policies via the FSMB (see below).
Created code of conduct templates for hospitals and medical groups, threatening termination or license referral for “contradictory public statements.”
Unprecedented shift:
Physicians’ free expression was reclassified as a form of medical misconduct.
The NBME & USMLE: Thought Policing Through Examination Content
Quiet but decisive role:
USMLE test content was swiftly updated to reflect current federal positions on virology, vaccination, and therapeutics.
Students who questioned vaccine efficacy, early treatment protocols, or official narratives on masking risked failing test questions explicitly designed to enforce the CDC line.
Step 1 and Step 2 practice resources added hundreds of new “clinical scenario” questions whose “correct” answers came directly from CDC guidance rather than emerging clinical literature.
Outcome:
Every future doctor became trained under ideological obedience testing: success required reproducing official doctrine verbatim.
This cemented conformity among medical trainees before they ever entered residency or independent research.
FSMB & State Licensing Boards: Real‑World Enforcement
By mid‑2021, the Federation of State Medical Boards (FSMB) issued its now‑infamous bulletin:
“Physicians who generate or spread COVID‑19 vaccine misinformation or disinformation risk disciplinary action by state medical boards, including suspension or revocation of their medical license.”
That sentence became a national standard within weeks:
At least 15 state boards copy‑pasted it into their rules.
Hospitals and employers adopted it as policy justification for firing dissenting staff.
Where did that text originate? From AMA counsel, reviewed by NBME and AAMC communications directors, and disseminated via FSMB channels.
Mechanism of coercion:
AAMC defines “misinformation” through curricular standardization.
AMA writes ethical justification for punishment.
FSMB codifies it into disciplinary regulations.
State boards enforce via legal penalties.
This was the guild system functioning exactly as intended — collective self‑preservation masquerading as “public health protection.”
Interaction with Federal Bureaucracies
The AAMC and AMA held biweekly coordination calls with HHS, CDC, and NIH starting spring 2020 to harmonize messaging.
Joint statements between AAMC–AMA–AHA (Hospitals) created mandatory “vaccine confidence campaigns.”
Academic researchers within AAMC institutions received NIH supplemental grants for “combating misinformation,” effectively turning research budgets into propaganda funding.
Information Control Feedback Loop:
AAMC generated “academic consensus” →
AMA validated it ethically →
HHS amplified it through media →
FSMB and NBME enforced compliance →
Dissenting doctors ostracized or silenced.
Suppression of Clinical Independence
There were thousands of instances of doctors sanctioned or threatened for:
Prescribing off‑label therapeutics (ivermectin, HCQ, etc.).
Citing data outside the NIH‑approved pool.
Discussing patient autonomy in vaccination decisions.
AAMC schools often pre‑emptively suspended privileges for hospital staff making “non‑aligned statements.” Behind those decisions were AAMC compliance memos referencing “threats to learning environment safety.” FSMB’s disciplinary coordination list (2021–2023) acted as a blacklist to prevent sanctioned physicians from re‑licensure in other states.
Financial Leverage and Research Bias
This web effectively wrote public‑health obedience into funding criteria, ensuring that non‑conforming schools or physicians were economically crippled. Each component reinforced institutional obedience with targeted financial control:
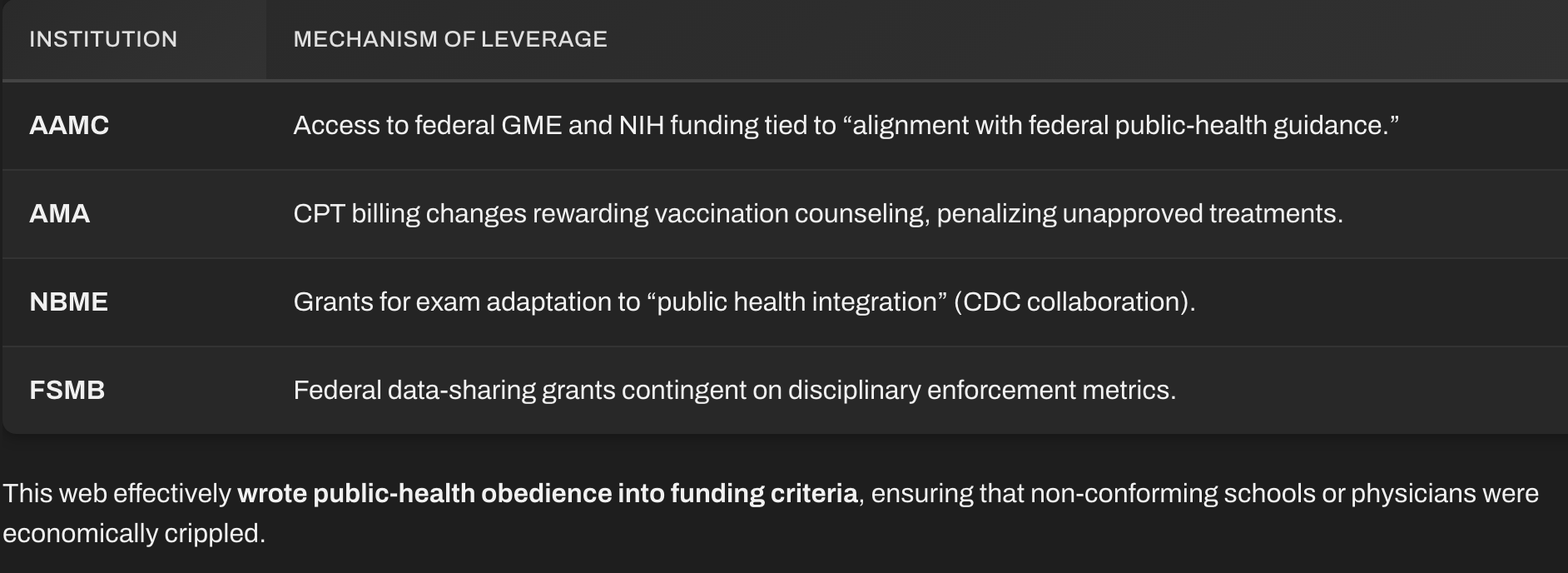
Structural Summary
AAMC → defines academic doctrine & provides media messagingAMA → codifies doctrine as ethics & policy; lobbies regulatorsNBME → tests belief compliance in students and traineesFSMB → criminalizes dissent through licensure enforcementState Boards → execute punishment at ground levelCDC/NIH/HHS → provide political endorsement and funding
All vectors converged on the same endpoint: a centralized command structure maintaining the illusion of widespread medical consensus.
Consequences
Elimination of Scientific Pluralism:
Alternative hypotheses or treatment approaches were delegitimized not by evidence, but by administrative decree.Erosion of Physician Autonomy:
Doctors became bureaucratic functionaries, not independent healers.Institutional Entrenchment:
The same apparatus remains today; repurposed for “disinformation” policing in all areas of medicine, not just COVID.Public Distrust:
Millions of Americans now know that “public health consensus” often means guild‑enforced unanimity rather than open scientific debate.
Aftermath and Current AAMC Initiatives
From Pandemic to “Climate‑Health Emergency”
AAMC’s pivot (2023–2025)
Created a Climate & Health Education Alliance with the National Academy of Medicine.
Reframed climate policy as a core public‑health competency, effectively replacing “pandemic preparedness” modules with “climate‑resilience training.”
Accreditation memos now require schools to demonstrate “climate‑impact awareness in curriculum,” which functions exactly as the former “vaccine‑confidence requirement.”
Key mechanism:
The same LCME standards once used to compel compliance with pandemic messaging now force curricular adoption of climate narratives—e.g., “carbon mitigation practices in hospital operations” and “environmental justice in health outcomes.”
Translation: COVID doctrine enforcement → environmental ideology enforcement.
AMA — Policy Codifier for Environmental Medicine
Published “Policy H‑135.985: Climate Change and Human Health.”
This commits the AMA to lobby for emissions reductions and “environmentally sustainable health systems.”Repurposed pandemic committees into “Climate Health Councils.”
Their function: write “ethical imperatives” to reduce carbon footprints—precisely the same moral framing once used for masking and vaccination.Distributed CPT code changes rewarding environmental data collection: hospitals log “carbon‑saving interventions” to meet CMS incentives.
Result: bureaucratic orthodoxies rewritten with new vocabulary—“carbon minimization” instead of “flatten the curve.” The AMA continues to define virtue through compliance.
NBME & Testing Infrastructure
Step 1/Step 2 exam banks now include “climate determinants of health” and “misinformation literacy.”
Question stems are drawn directly from UN IPCC–aligned claims about temperature and disease spread, presented as settled fact, not hypothesis.
Examinees must regurgitate sanctioned environmental talking points for passing grades.
Same structural function as pandemic testing: doctrinal reproduction through mandatory assessment.
FSMB & State Boards: “Online Conduct” Expansion
The Federation of State Medical Boards has extended its COVID “misinformation” bulletin into a permanent Professional Conduct framework:
“Physicians spreading disinformation in areas of public health importance (infectious disease, climate, emerging technoscience) may face disciplinary action.”
That add‑on: “emerging technoscience,” covers anything from AI policy to climate.
Boards are already citing it when reprimanding doctors who publicly dispute climate‑health claims or question government uses of AI diagnostics.
This is the same enforcement logic rewritten for new subject matter.
“AI Misinformation” – the Next Control Domain
Motivation:
Post‑COVID, mistrust in public health spiked. Rather than reopening debate, the guild complex reframed dissent as a cybersecurity problem.
Implementation (2024–2025):
AAMC & NBME: partnered with the Coalition for Trustworthy AI in Medicine (CTAiM).
Declared “AI literacy” a required competency.
Warns schools against “algorithmic misinformation” and “unvetted models,” i.e., non‑approved software or independent diagnostic tools.
AMA: issued policy H‑478.998 (“Professional Responsibility for the Use of AI in Medicine”), stating physicians must “critically appraise AI outputs consistent with authoritative guidance.”
“Authoritative guidance” = FDA or AAMC‑credentialed vendors.
FSMB: drafting rule language treating misuse of “unapproved digital tools” as unprofessional conduct.
Consequence: the new licensing frontier. A physician using an open‑source AI diagnostic or alternative therapy recommender can soon lose their license for violating “trust standards.”
This is the AI equivalent of prescribing ivermectin in 2021.
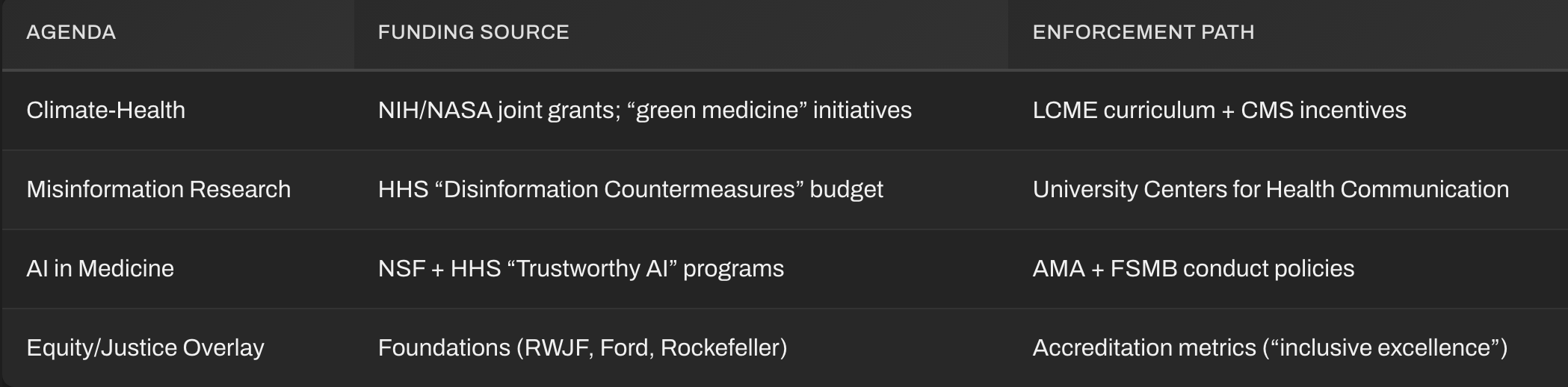
Funding and Bureaucratic Reinforcement
Each new narrative occupies the same bureaucratic pipeline that COVID once used.
Purpose and Effect
Preserve institutional legitimacy: shift focus from pandemic failure to a new moral frontier (“saving the planet,” “guarding data integrity”).
Maintain control mechanisms: accreditation, testing, licensure.
Insulate from political oversight: rebrand enforcement under broad “trust” or “sustainability” language.
Create perpetual emergency: environmental crisis replaces viral crisis as justification for centralized governance.
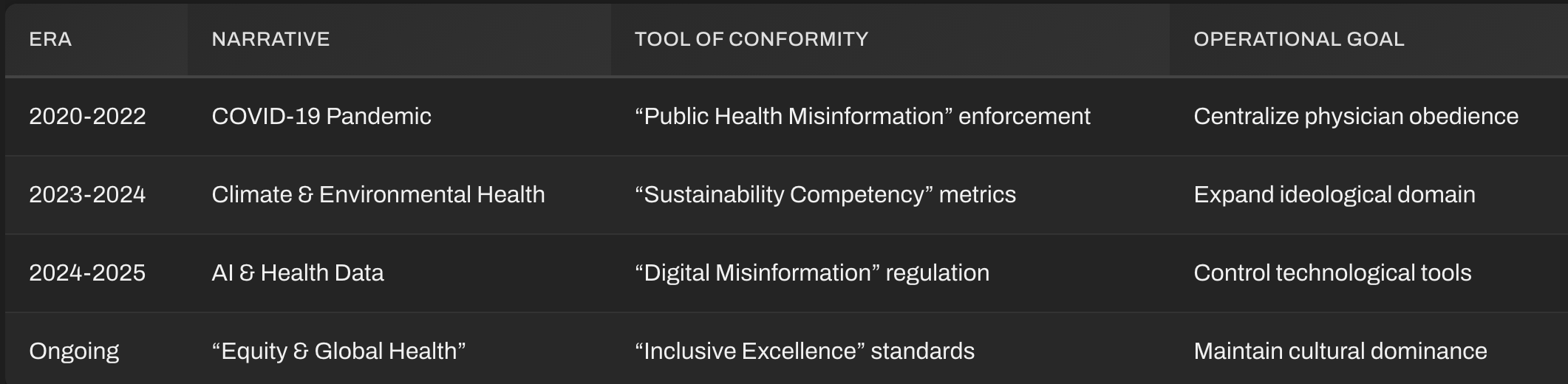
Conclusion
The Medical Guild complex now functions as a permanent medical Ministry of Information: whichever crisis replaces the last, the same channels distribute the doctrine, tie compliance to accreditation, and make deviation professionally suicidal.
The shocking reality of America’s healthcare system has been FULLY exposed now for the world to see since the 2020 pandemic. Functionally, the Illness Industrial Complex’s Deep State allies waged a massive war on healing. AAMC, in cooperation with Big Pharma, corporate media, and a globalized censorship-industrial complex employing military-grade psychological warfare technologies weaponized medical boards against truth-telling doctors and whistleblowers.
The corruption of modern medicine has reached systemic proportions, with manipulation of medical literature and research funding constituting not mere ethical failure but potential criminal conspiracy under RICO statutes. Secretary of Health RFK Jr now says that President Trump’s Department of Justice will launch RICO investigations to go after and prosecute the collusion between the scientific community, medical boards, medical journals, and Big Pharma.
Corporate interests have infiltrated the National Institutes of Health and other health agencies, transforming American medical research into a profit‑driven racket that sacrifices truth and public well‑being for institutional enrichment. What now exists is not a health system but a Medical Industrial Complex built around a medieval Guild business model, which functions as a shadow government, controlling data, policy, and discourse to preserve its power. The only viable remedy is a complete structural overhaul led by the Department of Justice to dismantle this Guild cartel, purge corporate influence from scientific oversight, and restore medicine to its rightful purpose: serving the health and freedom of the American people.
Obesity is a perfect example that ties to the AAMC and pharma. STAT covered this story back in 2023 but for the longest, obesity was a lifestyle choice. However, medical schools began to see obesity as a disease, not lifestyle, so that drugs, GLPs, could be used for this disease: https://unorthodoxy.substack.com/p/the-hidden-struggle-in-health-care
MAHA has brought this expose to light and that was just year one. Hoping this continues for the next three years to complete upend this “open‑ended ideological governance over medicine itself.”
Attorneys have the exact same problem with the American Bar Association.