
Treating the Wound, Not the Textbook
Why chronic diabetic and low-circulation wounds call for a different approach

Adjunct Professor Robert W. Malone, MD, MS.
Chief Medical Officer, Curativa Bay - www.curativabay.com
For most of my career, I have studied (and taught hundreds of medical students) pathology, infectious disease, immunology, and how cells respond to injury. One lesson keeps returning, and it is simple enough to sound obvious: the environment in which you treat an infection changes, which treatments succeed and which fail. A medicine that performs beautifully in one setting can underperform badly in another, not because the medicine is bad, but because the biology around it has changed.
Nowhere is this clearer than in the treatment of diabetic foot ulcers and other low-circulation wounds. These wounds are common, they cause enormous suffering, and they lead to amputation at rates we should find unacceptable. For decades, we have treated them, in large part, with tools designed for a very different kind of wound. The story of how that happened says something useful about how medicine actually changes and points toward an approach available today but still uncommon.
The Pathophysiology That Changes Everything
A diabetic foot ulcer is not a simple cut that happens to be infected. It is a chronic infection sitting inside tissue that has lost much of its ability to defend and repair itself. Several problems arrive at once. Blood flow is reduced by disease in the small and large vessels, so the tissue is starved of oxygen. High blood sugar weakens the immune response directly, blunting the cells that would normally clear an infection. Nerve damage means a person often cannot feel the wound forming until it is advanced. And the inflammation of diabetes tends to smolder rather than resolve. [3,4]
Into this weakened environment, bacteria settle in. They rarely remain as free-floating cells that antibiotics can easily reach. Instead, they build biofilms, communities of microbes wrapped in a self-made matrix of sugars, proteins, and DNA. Inside a biofilm, bacteria become far harder to kill. Laboratory studies have shown biofilm populations tolerating antibiotic concentrations up to a thousand times higher than their free-floating counterparts. [5] The matrix shields them from the immune system, and a fraction of the population drops into a dormant, persister state that most antimicrobials cannot touch. When treatment stops, those survivors regrow. [6] This is the engine of a chronic wound.
Why Silver Was Built for a Different Wound
For decades, the front-line dressings for these wounds have relied on silver, usually as silver sulfadiazine or a silver-impregnated dressing. Silver works, and there is a good reason it became standard. But it is worth remembering what it was built for. Silver sulfadiazine was introduced in 1968 as a treatment for burns. [7] The burn was an ideal proving ground: common, severe, with a defined course and quick, measurable outcomes.
A burn and a diabetic ulcer, though, are almost opposites. The burn patient usually has an intact immune system and reasonable circulation, and the wound is acute, expected to resolve over days to weeks. The aim is fast sterilization while the body’s own healing machinery is still running. A diabetic foot ulcer reverses nearly every one of those conditions: the immune system is impaired, the circulation is poor, and the wound is chronic. [3,4] Reaching for a burn-era tool here is not unreasonable on its face. It is simply a different problem.
Why Silver Struggles in Chronic Wounds
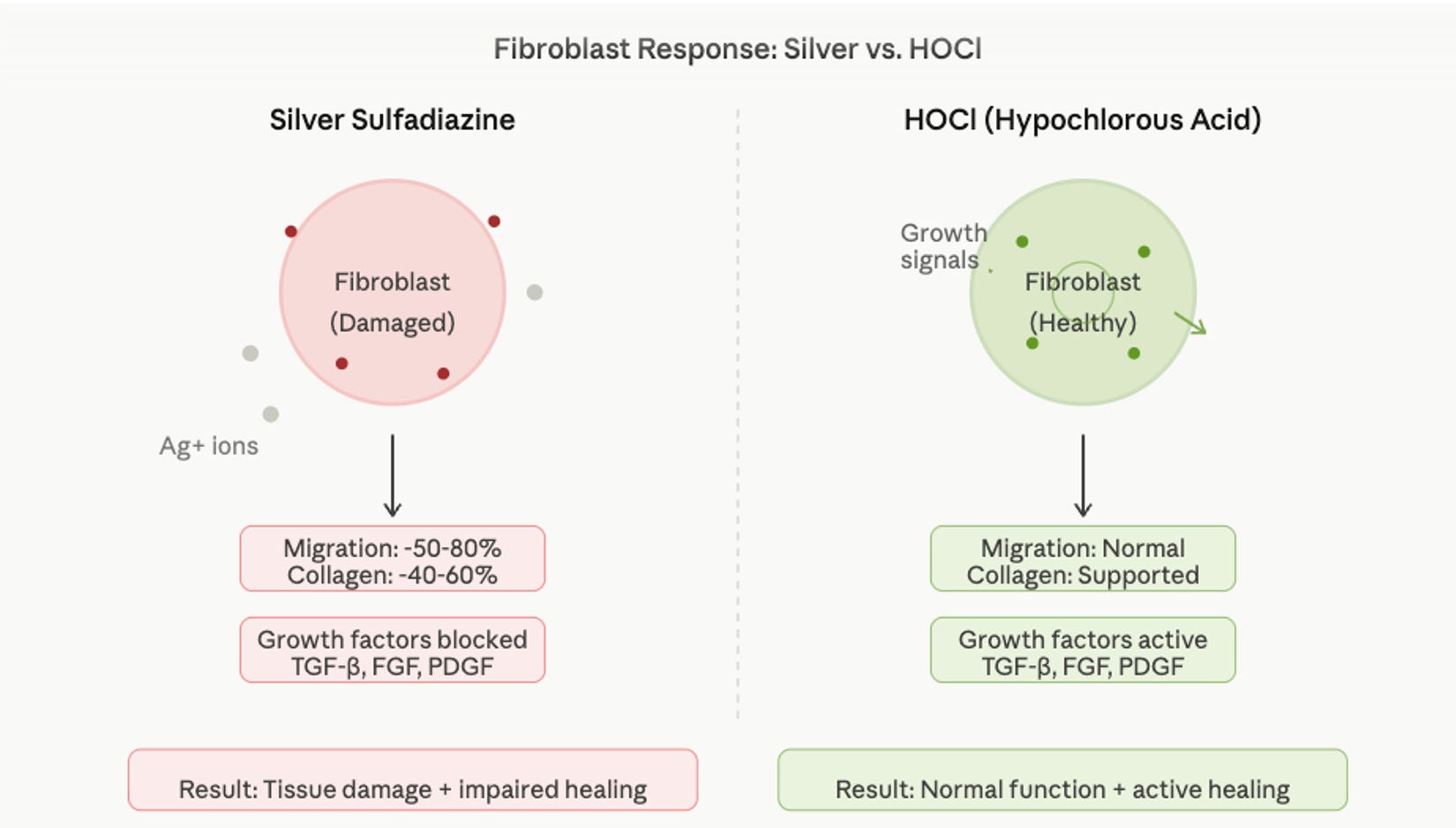
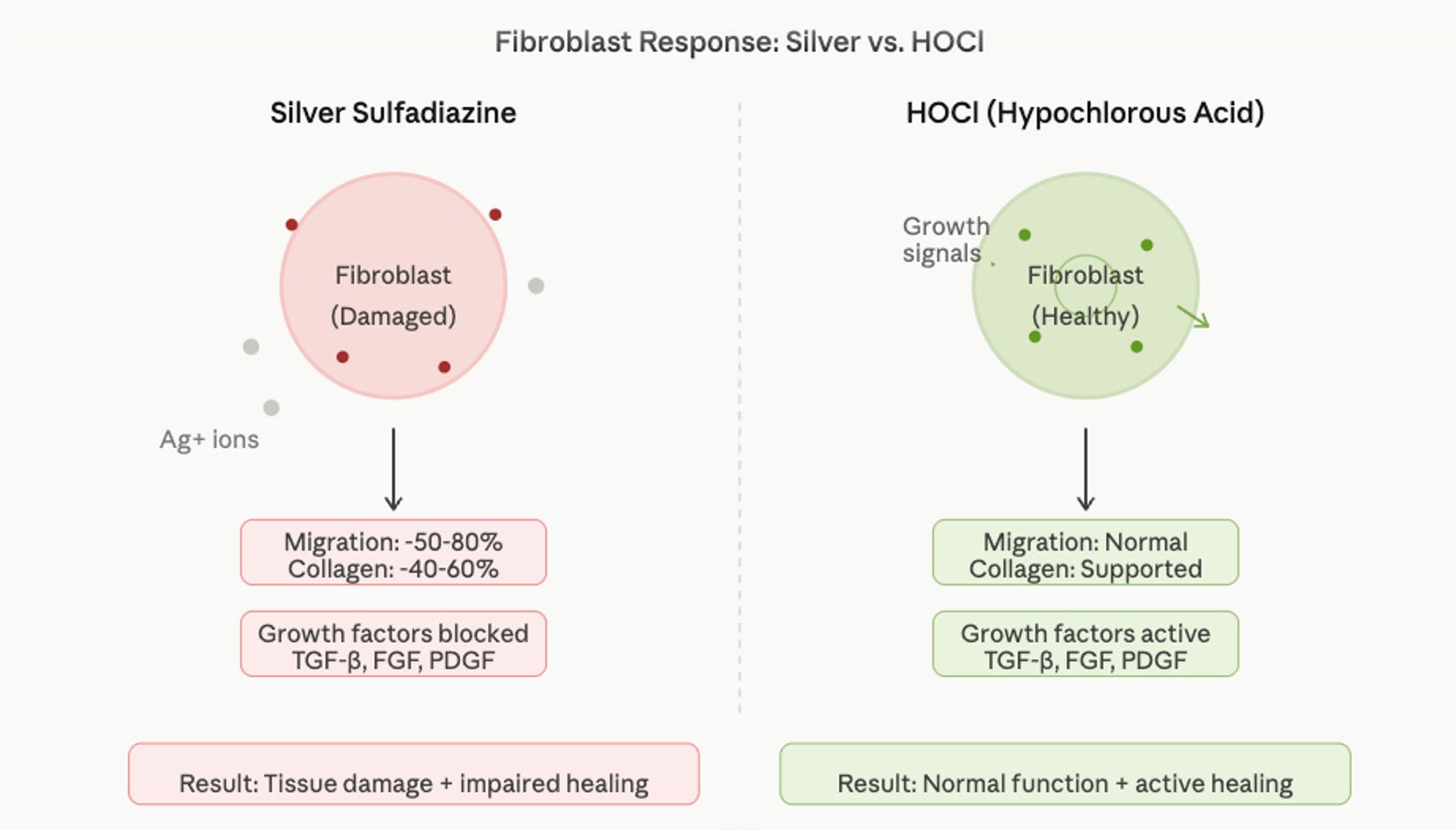
Silver kills microbes through oxidation: it disrupts their membranes, binds essential proteins, and interferes with respiration. [8] The difficulty is that this chemistry is not selective. The same reactions that harm bacteria can also harm human cells, and in laboratory studies the cells most affected are the ones a chronic wound needs most. Fibroblasts build the collagen scaffold of new tissue, and keratinocytes resurface it. In cell culture, silver is toxic to both, with fibroblasts especially sensitive, impairing their survival and their ability to migrate and lay down collagen. [9,10] This sets up a real tension: the concentration that controls infection may also slow the repair you are trying to support.
Candor requires a caveat. What happens in a culture dish does not always predict what happens in a living wound. In at least one careful comparison, several silver dressings were clearly toxic to fibroblasts in the laboratory yet still accelerated healing in an animal model, because a living wound is a far more complex place than a layer of cells in a dish. [10] Silver is not useless. The argument is narrower and more interesting: in the particular setting of a chronic, biofilm-laden, poorly perfused wound, the balance of benefit and harm can tip the wrong way.
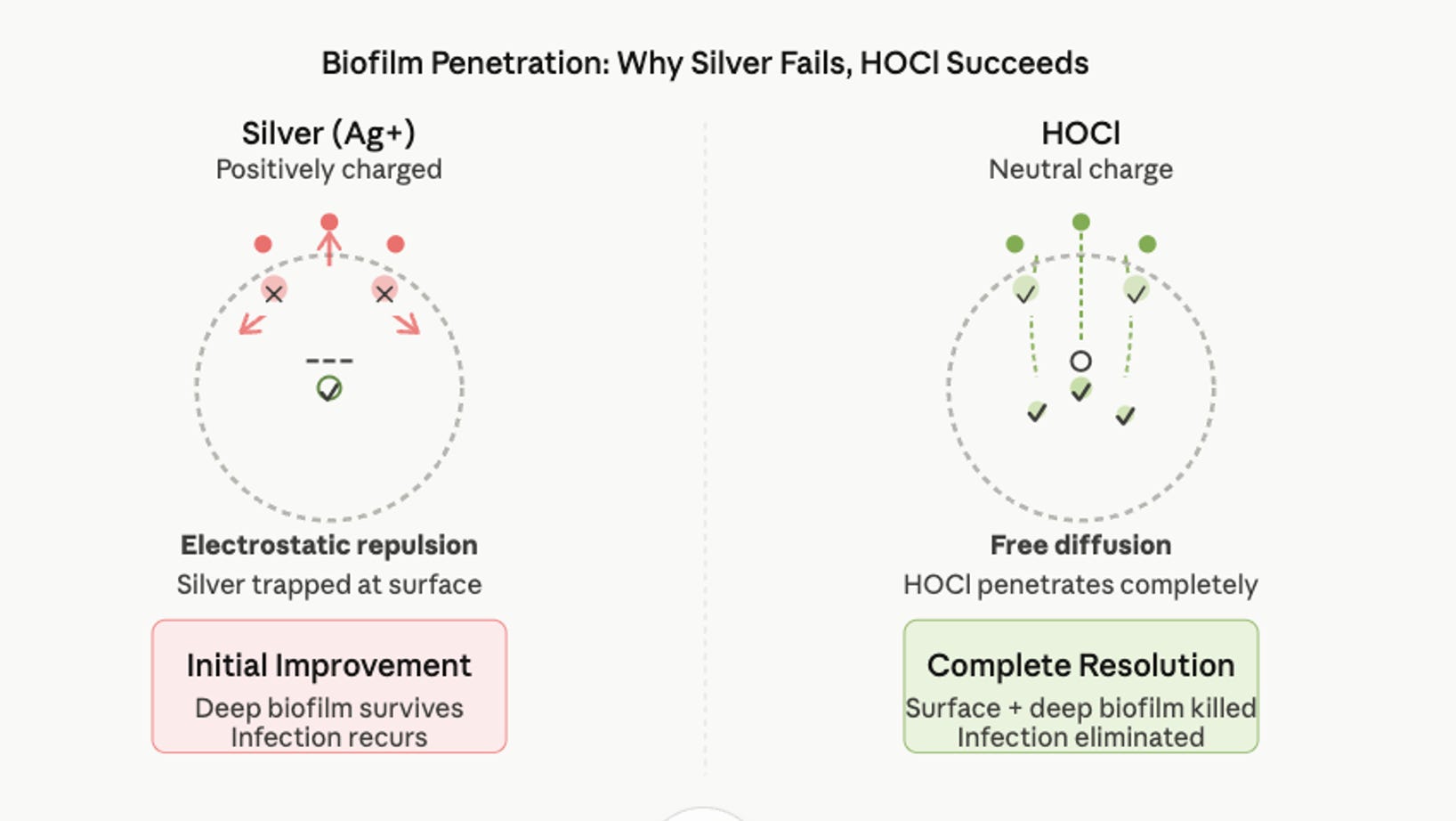
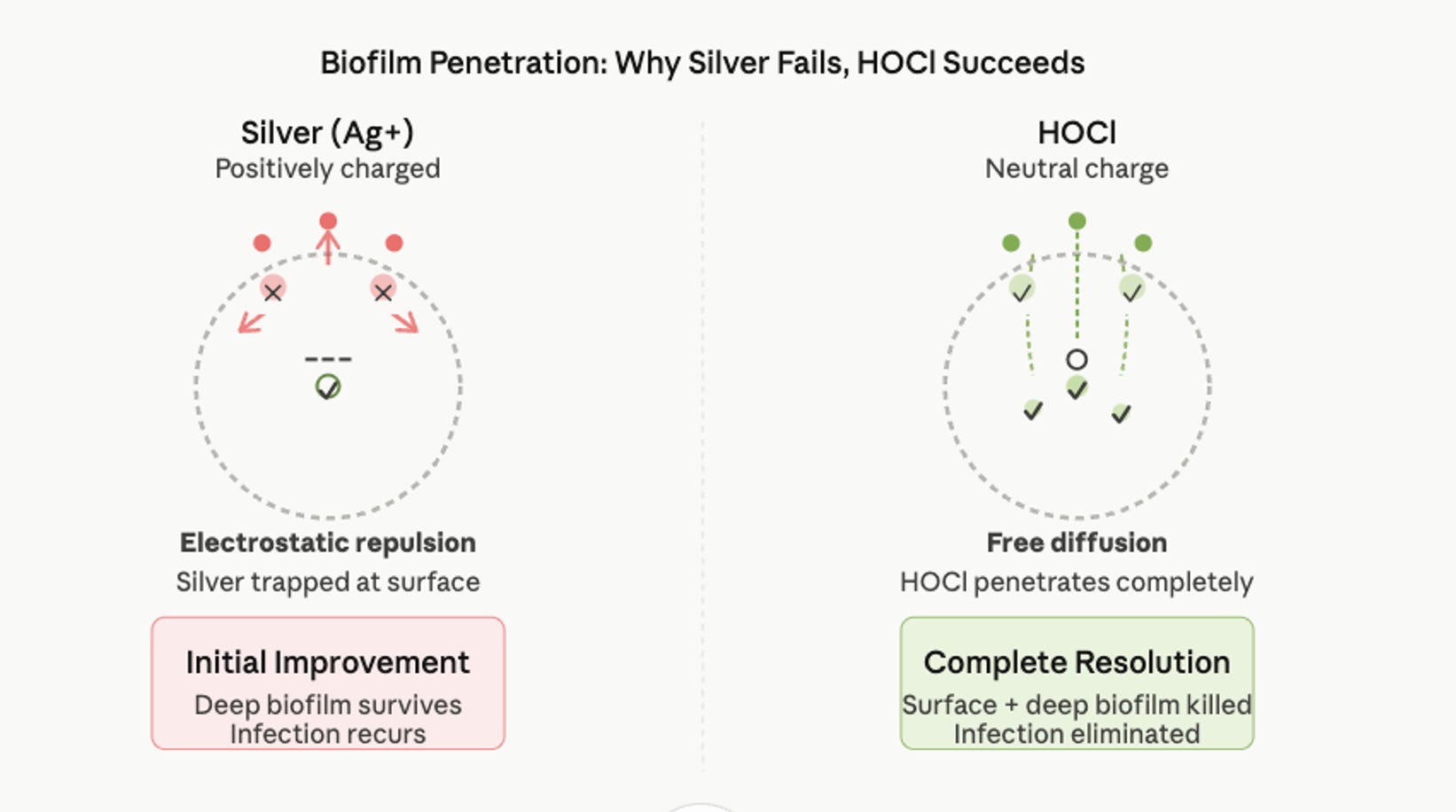
A second problem matters especially for biofilm. To kill bacteria, an antimicrobial first has to reach them, and the biofilm matrix is good at preventing that. The matrix can bind and hold antimicrobial agents near its surface, and how well an agent penetrates depends heavily on its size and electrical charge. [11,12] When the surface bacteria die while the deeper, protected cells survive, a wound can look better for a few weeks and then relapse, a pattern familiar to anyone who treats these ulcers. [6]
A third concern is the blood supply itself. Diabetic wounds, especially those with poor circulation, depend on growing new blood vessels to restore oxygen. That process runs through endothelial cells, which line blood vessels and must multiply and migrate to form new capillaries. The oxidative chemistry that troubles fibroblasts can affect endothelial cells as well, and impaired new-vessel formation is among the best-documented reasons diabetic wounds fail to heal. [13,14] Povidone-iodine and chlorhexidine, the other common antiseptics, carry their own versions of this tradeoff between killing power and tissue tolerance. [17]
Why the Practice Persists
If the case against silver in chronic wounds is reasonable, why does it remain standard? The honest answer is mostly inertia, not conspiracy. Silver earned its place in burn care in the 1970s and 1980s on solid evidence. Regulatory clearances, reimbursement, clinician training, and whole product lines were built around it. When diabetic foot ulcers grew into a major problem, the natural move was to reach for the dressings already on the shelf.
Changing a standard of care is difficult. It takes well-designed trials, updated guidelines, retraining, and a willingness among payers to cover something new. Incentives also matter. Large, independent, head-to-head trials are expensive, and there tends to be more commercial enthusiasm for premium products than for simple, inexpensive ones. None of this requires bad intent. It only requires a system that changes slowly, which every medical system does.
Why Low-Circulation Wounds Are Different
It is worth pausing on why poor circulation changes the whole equation. In a normally perfused wound, the immune system can do much of the work: white blood cells reach the site, clear bacteria, and the repair cascade proceeds, even if slowly. In a low-circulation wound, the blood cannot deliver enough oxygen, nutrients, or immune cells. You cannot rely on the body to contain the infection on its own, and you cannot wait for a healing cascade that is starved of what it needs. [13]
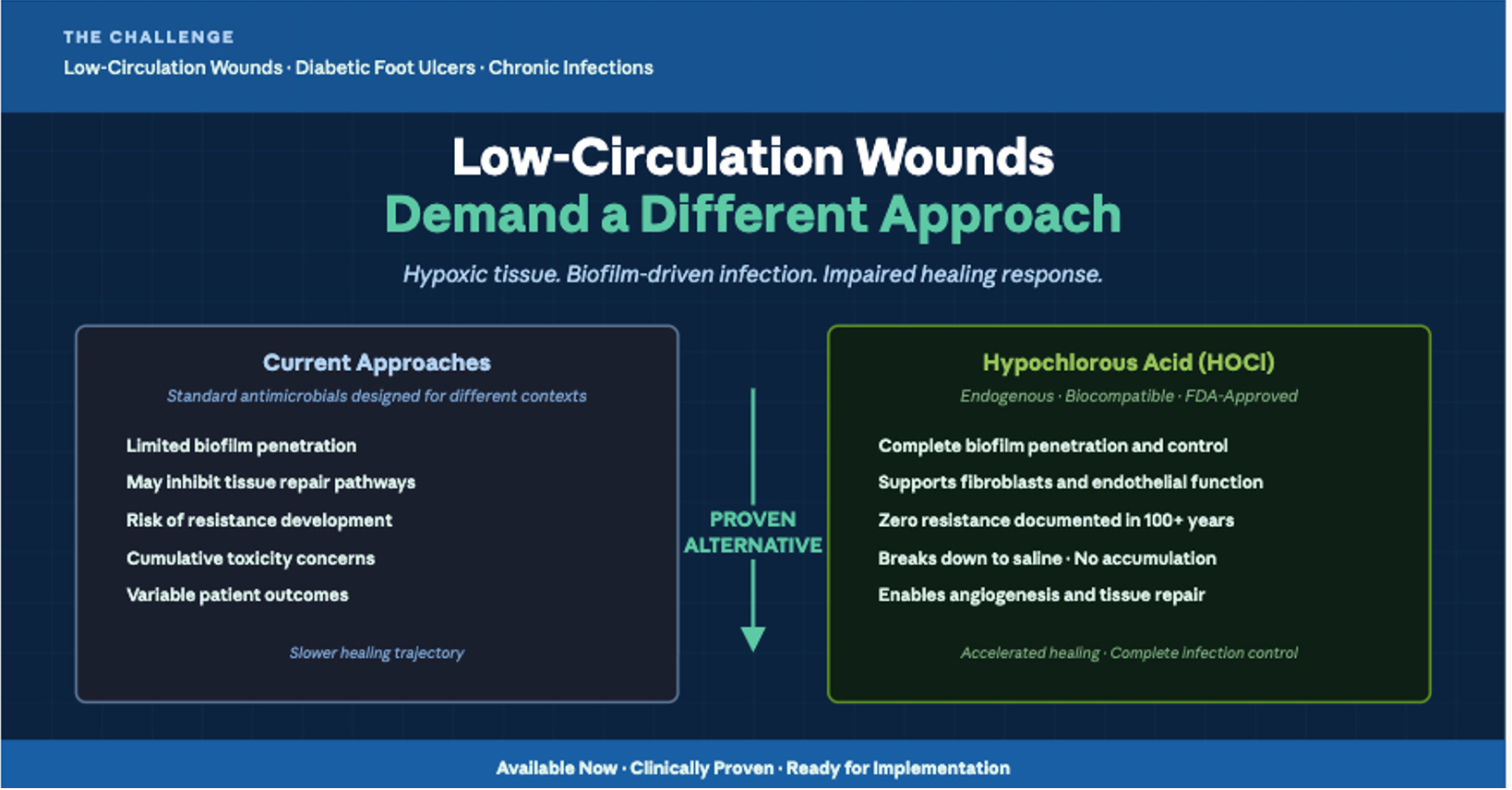
That leaves a demanding wish list for any treatment. It should penetrate biofilm rather than be turned away at the surface. It should kill a broad range of microbes quickly. It should spare fibroblasts, keratinocytes, and endothelial cells rather than damage them. It should not build up in tissue with repeated use, and it should not breed resistance. Silver and the older antiseptics meet only some of these. One option meets most of them, and it is not a new invention at all. It is a molecule the body already makes.
Hypochlorous Acid: A Molecule the Body Already Makes
When a white blood cell engulfs a microbe, it mounts a chemical attack. An enzyme called myeloperoxidase combines hydrogen peroxide with chloride to produce hypochlorous acid, written HOCl. [15,18] This is one of the body’s own front-line antimicrobial weapons, refined by evolution to kill pathogens inside tissue that still needs to survive and heal. Stabilized HOCl solutions take that same molecule and make it shelf-stable for use on wounds. [15]
This pedigree is not only biological. It is also clinical, and surprisingly old. During the First World War, long before antibiotics existed, the chemist Henry Drysdale Dakin developed a dilute, buffered sodium hypochlorite solution to cleanse the heavily contaminated wounds of the battlefield, delivered by the continuous irrigation approach known as the Carrel-Dakin method. [23,24] The active antimicrobial species that solution releases in tissue is hypochlorous acid itself. [23] A chlorine-based oxidant chemistry, with HOCl at its heart, was therefore already saving limbs and lives a century ago. Its use faded after penicillin became established in the 1940s, not because it had failed, but because a systemic antibiotic taken by mouth or injection was simply more convenient than a solution that had to be freshly prepared and applied again and again. [24] Those early solutions were also chemically unstable and lost their potency within days. [24] What modern stabilization adds is the part the wartime chemists could not solve: it delivers the same active molecule in a shelf-stable, pH-balanced, and far less irritating form.
This is not a fringe or experimental idea. Stabilized hypochlorous acid is cleared by the United States Food and Drug Administration for cleansing, irrigating, and debriding both acute and chronic wounds, including diabetic ulcers and burns. [19] Its relative obscurity in everyday practice owes more to habit and marketing than to any real question about whether it is permitted or safe.
How It Works Against Bacteria and Biofilm
HOCl is a small, uncharged molecule, and that turns out to matter. Carrying no charge, it is not repelled by the biofilm matrix the way some agents are, so it can diffuse into the biofilm rather than being held at the surface. [12,17] Once inside, it attacks microbes on several fronts at once: it oxidizes their membranes, inactivates essential enzymes, and damages their nucleic acids. [15]
This many-targets-at-once quality is the key to a claim worth stating carefully. Because HOCl strikes so many essential systems simultaneously, the evolutionary path to resistance is far narrower than for a medicine that hits a single target, and clinically meaningful resistance has not emerged in practice. [15,16] That is a strong statement, but it is not the same as saying resistance is impossible; it is saying the odds are stacked heavily against it. In practical terms, HOCl acts quickly against bacteria, viruses, and fungi, and it can disrupt biofilm, which is precisely the obstacle that defeats so many other agents in these wounds. [16,17]
How It Spares Healing Tissue
The more elegant part is what HOCl does not do. Because the body produces it, human tissue has evolved defenses against it. Our cells carry antioxidant systems that neutralize HOCl at the concentrations used in wound care, so it can lower the bacterial burden without crippling the cells that rebuild tissue. [16] Laboratory and clinical work supports this difference: where harsher antiseptics suppress fibroblasts and keratinocytes, HOCl is comparatively gentle on them and has been associated with re-epithelialization, the resurfacing of the wound. [16,18] The same logic extends to endothelial cells, and therefore to the formation of new blood vessels. [16]
Why This Matters for New Blood Vessels
Here is the heart of why chronic diabetic wounds are their own category. When tissue runs short of oxygen, it switches on a signaling protein called HIF-1 alpha, which drives the release of vascular endothelial growth factor, or VEGF. VEGF tells endothelial cells to multiply and build new capillaries. Those vessels deliver oxygen, oxygen lets fibroblasts lay down collagen, and the wound can finally close. In diabetes, this cascade is already impaired, which is a major reason these wounds stall. [13,14] Any treatment that further damages endothelial cells works against the one process the wound most needs. A treatment that leaves them intact gives the cascade a chance to proceed. [16]
How It Is Used
In practice, HOCl is usually applied by irrigating the wound with the solution, allowing it to remain in contact with the wound bed, and then covering the wound with an appropriate dressing. The appeal is its simplicity. It needs no specialized equipment or complex supply chain, and because it does not accumulate in tissue, it can be used frequently without the buildup seen with some other agents. Prolonged use of silver, by contrast, can deposit silver in the skin and produce a blue-gray discoloration known as argyria. The specifics of how often and exactly how a given wound should be treated are clinical judgments that belong to a person’s own care team, not to an essay.
What the Evidence Shows, and What It Does Not
It is important to be candid about the strength of the evidence, because that candor is part of the argument. The mechanistic case for HOCl is strong and well understood. The clinical case is promising but still maturing. Small, randomized studies, observational studies, and case reports in diabetic and chronic wounds have reported reduced bacterial burden, less pain and odor, and improved healing compared with conventional antiseptics. [20,21,22] Several of these studies are small, and some appear in lower-tier journals, so they are best read as encouraging rather than conclusive.
What is missing is the large, independent, multicenter randomized trial that would settle the question beyond a reasonable doubt, ideally a direct comparison against silver in chronic diabetic wounds. The absence of that one landmark study is not the same as an absence of evidence. The biology is coherent, the smaller studies point in a consistent direction, and the safety profile is favorable. Intellectual honesty simply means saying plainly that the definitive trial has not yet been done. Despite this lack of large, randomized clinical trials, many cutting-edge burn and wound clinics routinely use HOCl in the clinical treatment of these ulcers. Strangely, this adoption appears to be more widespread in Canada than in the United States.
Why It Matters
Diabetic foot ulcers are common. In the United States alone, there are over a million active diabetic foot ulcers at any given time. Globally, the prevalence is far higher.
These ulcers cause suffering. They lead to infection. They lead to amputation. A diabetic patient who loses a foot faces a profoundly altered life. The mortality risk increases. The disability is permanent.
We have better tools available now. Not perfect tools. Nothing is perfect. But better tools, based on a more accurate understanding of the pathophysiology of chronic diabetic wounds. Yet these tools remain uncommon in practice.
The stakes here are not abstract. Each year in the United States roughly 1.6 million people develop a diabetic foot ulcer, and these wounds precede the large majority of diabetes-related amputations. [1] The figures that follow a major amputation are sobering: five-year mortality estimates commonly fall between 50 and 70 percent, worse than for many cancers, and recurrence is common even after a wound heals. [1,2]
American Physicians, Medical practitioners, and Nurses are not short on compassion for these patients. We may, in some cases, be short on matching the tool to the biology. The argument of this essay is narrow and, I hope, fair. The chronic, poorly perfused, biofilm-laden diabetic wound is a clinically important problem, and there is a strong physiological case, supported by a growing body of clinical work, for an approach centered on a molecule that the immune system already uses. The remaining barrier is neither safety nor permission. It is the slow pace at which good ideas become common practice, and the trials still needed to push them there.
Why have we not seen more rapid uptake of HOCl into clinical practice in the USA?
Because institutions are slow to change. Because financial incentives point the wrong direction. Because clinical inertia is powerful.
This is not a scandal of malice. It is a scandal of neglect. Nobody set out to use suboptimal treatments for diabetic wounds. It is simply that better treatments exist but have not been widely adopted because the pathway for adoption is hard.
Look north, however, and the picture changes. In Canada, stabilized hypochlorous acid has moved further into routine wound care than it has in the United States. Several HOCl wound products are licensed by Health Canada as medical devices, some of them manufactured domestically in Ontario, and they are stocked and distributed through the same hospital supply channels that carry conventional dressings. [25,26]
The national wound-care community has taken them up as well. Wounds Canada, the country’s professional wound-care organization, has featured pure hypochlorous acid cleansers in its educational materials, and the approach is in use at centers such as the Limb Preservation Clinic at The Ottawa Hospital. [27] This does not mean Canadian practice is uniform, and some of the most enthusiastic language comes from manufacturers rather than from independent audits. But the lesson is hard to miss. A comparable health system, facing the same biology and the same patients, has folded this molecule into ordinary care. And on the international front, the WHO now lists HOCl as an essential medicine. The American lag is therefore a choice, not a law of nature, and choices can be revisited.
But the better treatment is there. It works. It is less toxic. It is cheaper. It causes less pain. It enables healing of these types of wounds in a way that silver cannot.
For any clinician treating diabetic foot ulcers, the question is not whether to use HOCl. It is whether to continue using silver when the evidence and the physiology both point toward a better choice.
For any patient with a diabetic foot ulcer that is not healing, the question is worth asking: has my clinician considered HOCl? Or are we stuck with protocols designed for acute burns because that is how we have always done it?
The physiology of chronic diabetic wounds is distinct. The treatment should be distinct. The tool exists. The evidence supports it. The barrier is only inertia.
That barrier can be overcome. It needs to be overcome. The cost of not overcoming it is measured in lost limbs and shortened lives.
References
1. McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2023;46(1):209-221.
2. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. New England Journal of Medicine. 2017;376(24):2367-2375.
3. Pouget C, Dunyach-Remy C, Pantel A, Schuldiner S, Sotto A, Lavigne JP. Biofilms in diabetic foot ulcers: significance and clinical relevance. Microorganisms. 2020;8(10):1580.
4. Afonso AC, Oliveira D, Saavedra MJ, Borges A, Simoes M. Biofilms in diabetic foot ulcers: impact, risk factors and control strategies. International Journal of Molecular Sciences. 2021;22(15):8278.
5. Hall CW, Mah TF. Molecular mechanisms of biofilm-based antibiotic resistance and tolerance in pathogenic bacteria. FEMS Microbiology Reviews. 2017;41(3):276-301.
6. Yan J, Bassler BL. Surviving as a community: antibiotic tolerance and persistence in bacterial biofilms. Cell Host and Microbe. 2019;26(1):15-21.
7. Fox CL Jr. Silver sulfadiazine, a new topical therapy for Pseudomonas in burns. Archives of Surgery. 1968;96(2):184-188.
8. Fox CL Jr, Modak SM. Mechanism of silver sulfadiazine action on burn wound infections. Antimicrobial Agents and Chemotherapy. 1974;5(6):582-588.
9. Poon VKM, Burd A. In vitro cytotoxicity of silver: implication for clinical wound care. Burns. 2004;30(2):140-147.
10. Burd A, Kwok CH, Hung SC, et al. A comparative study of the cytotoxicity of silver-based dressings in monolayer cell, tissue explant, and animal models. Wound Repair and Regeneration. 2007;15(1):94-104.
11. Sequestration of nanoparticles by an EPS matrix reduces the particle-specific bactericidal activity. Scientific Reports. 2016;6:21379.
12. pH-responsive, charge-reversing layer-by-layer nanoparticle surfaces enhance biofilm penetration and eradication. 2024. PMC11117027.
13. Bitar MS, Al-Mulla F. Upregulation of CREM/ICER suppresses wound endothelial CRE-HIF-1 alpha-VEGF-dependent signaling and impairs angiogenesis in type 2 diabetes. Disease Models and Mechanisms. 2014;7(12). doi:10.1242/dmm.017145.
14. Angiogenesis during diabetic wound repair: from mechanism to therapy opportunity. Burns and Trauma. 2024. doi:10.1093/burnst/tkae052.
15. Wang L, Bassiri M, Najafi R, et al. Hypochlorous acid as a potential wound care agent: part I. Journal of Burns and Wounds. 2007;6:e5.
16. Robson MC, Payne WG, Ko F, et al. Hypochlorous acid as a potential wound care agent: part II. Its role in decreasing tissue bacterial bioburden and overcoming the inhibition of infection on wound healing. Journal of Burns and Wounds. 2007;6:e6.
17. Antimicrobial efficacy of a very stable hypochlorous acid formula compared with other antiseptics used in treating wounds: in-vitro study on micro-organisms with or without biofilm. Journal of Hospital Infection. 2020.
18. Hypochlorous acid: applications in dermatology. Journal of Integrative Dermatology.
19. U.S. Food and Drug Administration. 510(k) premarket notification K123072: Vashe Wound Therapy Solution. 2013.
20. The effectiveness of hypochlorous acid solution on healing of infected diabetic foot ulcers (randomized comparison versus hydrogen peroxide and povidone-iodine). Journal of Education and Practice. 2017. ERIC EJ1139092.
21. A retrospective health economic analysis of a stable hypochlorous acid preserved wound cleanser versus 0.9 percent saline as instillation for negative-pressure wound therapy in severe and infected wounds. 2022. PMC9123387.
22. The use of hypochlorous acid in the healing of a diabetic foot ulcer (case studies). International Journal of Biomedical Engineering and Clinical Science. 2022.
23. Dakin solution. In: StatPearls. Treasure Island (FL): StatPearls Publishing; updated 2023. NCBI Bookshelf NBK507916.
24. Dakin HD. On the use of certain antiseptic substances in the treatment of infected wounds. British Medical Journal. 1915.
25. Medline Canada. Vashe Hypochlorous Acid (HOCl) Wound Solution and BIHOCL PureCleanse Wound Cleanser (product listings). medline.ca.
26. Biomiq Inc. BIHOCL and PureGel hypochlorous acid wound products (Health Canada Class II licensed medical devices). Kitchener, Ontario; 2025.
27. Presentation digests on pure hypochlorous acid wound cleansers. Wound Care Canada (Wounds Canada). 2022-2023. woundscanada.ca.
Medical Disclaimer
This essay is provided for general educational and informational purposes only. It is not medical advice and is not a substitute for diagnosis or treatment by a qualified health professional. Wound care decisions, including the choice of any dressing or antiseptic, depend on the individual and should be made together with a licensed clinician who can examine the wound and weigh the full medical picture. If you or someone you care for has a wound that is not healing, that shows signs of infection, or that is associated with diabetes or poor circulation, please seek care from your own medical provider. Do not delay or disregard professional medical advice because of something you have read here.
Wow, this article is amazing. Thank yo so much. I have been an insulin diabetic for 43 years and fortunately I have had no major issues. I will say, I work hard at control and exercise almost daily. I have not eaten an entire candy bar for 43 years. I can make a Snickers bar last for 2 weeks (when I have a craving I cut off a little piece and enjoy). Thank you for this information. I will save it in case I ever need it. When I was diagnosed, I told myself I came in with 4 limbs and I will go out with four limbs.
Thank you for this article, Dr Malone. My husband is a type II diabetic but is under control with metformin, diet and exercise. We watch his feet carefully and his left great toenail became loose, we think from wearing Wellington boots when the yard was wet. It has stopped growing although it appears to be attached at the sides again. He has gone to his podiatrist twice to have it examined at my insistence, but the podiatrist is not concerned. There is no redness or swelling. I did buy Curativa Bay HOCL for skin problems when you first wrote about it. I am going to try it on his toe just see if it helpful in restoring the growth of the nail.
BTW, I have neuropathy from a vaccine injury(Shingrix). I use DMSO to relieve the painful spasms associated with it. It’s amazing!