
WHAT YOUR COVID BOOSTER DID TO YOUR IMMUNE SYSTEM
A plain-language guide to what the research now shows


What this is about
If you got multiple COVID-19 booster shots, something happened to your immune system that your doctor probably never mentioned, and that your post-vaccination blood test almost certainly cannot detect.
A growing body of peer-reviewed research published between 2023 and 2025 documents that repeated mRNA boosting causes a progressive shift in the type of antibody your immune system produces against the virus. This shift is not random noise. It follows a well-understood biological pattern. And it has measurable, functional consequences.
This article explains what that shift is, what it means, who it matters most for, and what should be done about it. No prior immunology background is required.
The standard post-vaccination blood test that tells you how much antibody you have says nothing about what kind of antibody you have. After multiple boosters, that distinction matters.
Not all antibodies are the same
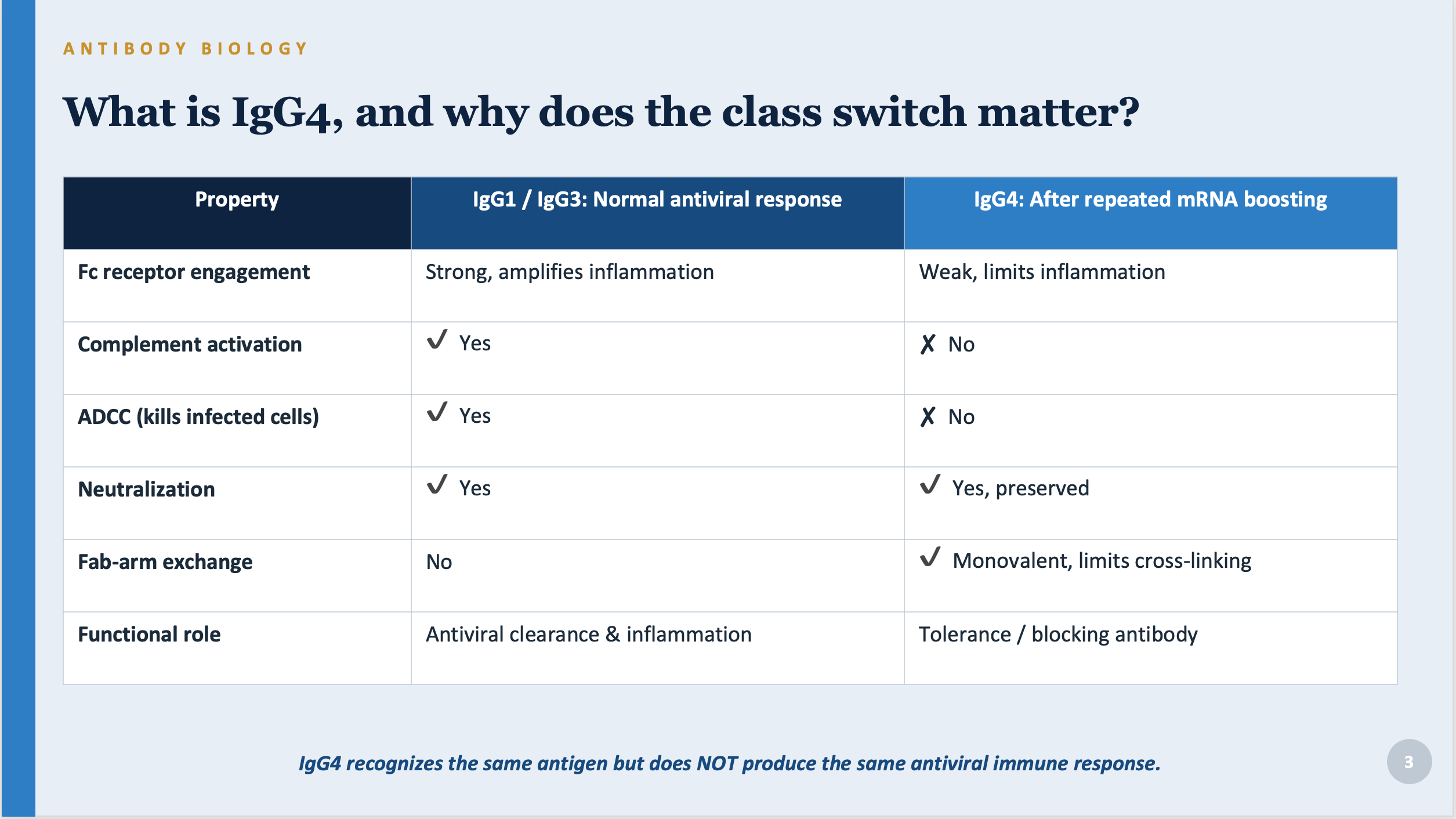
Your body makes several types of antibodies, labeled IgG1 through IgG4. When you encounter a virus or receive a vaccine for the first time, your immune system mostly produces IgG1 and IgG3. These are your fighter antibodies. They do two key things:
• They block the virus from entering your cells (this is called neutralization).
• They recruit other immune cells to find and destroy cells the virus has already infected. This second function is called ADCC (antibody-dependent cellular cytotoxicity), and it depends on a part of the antibody called the Fc region.
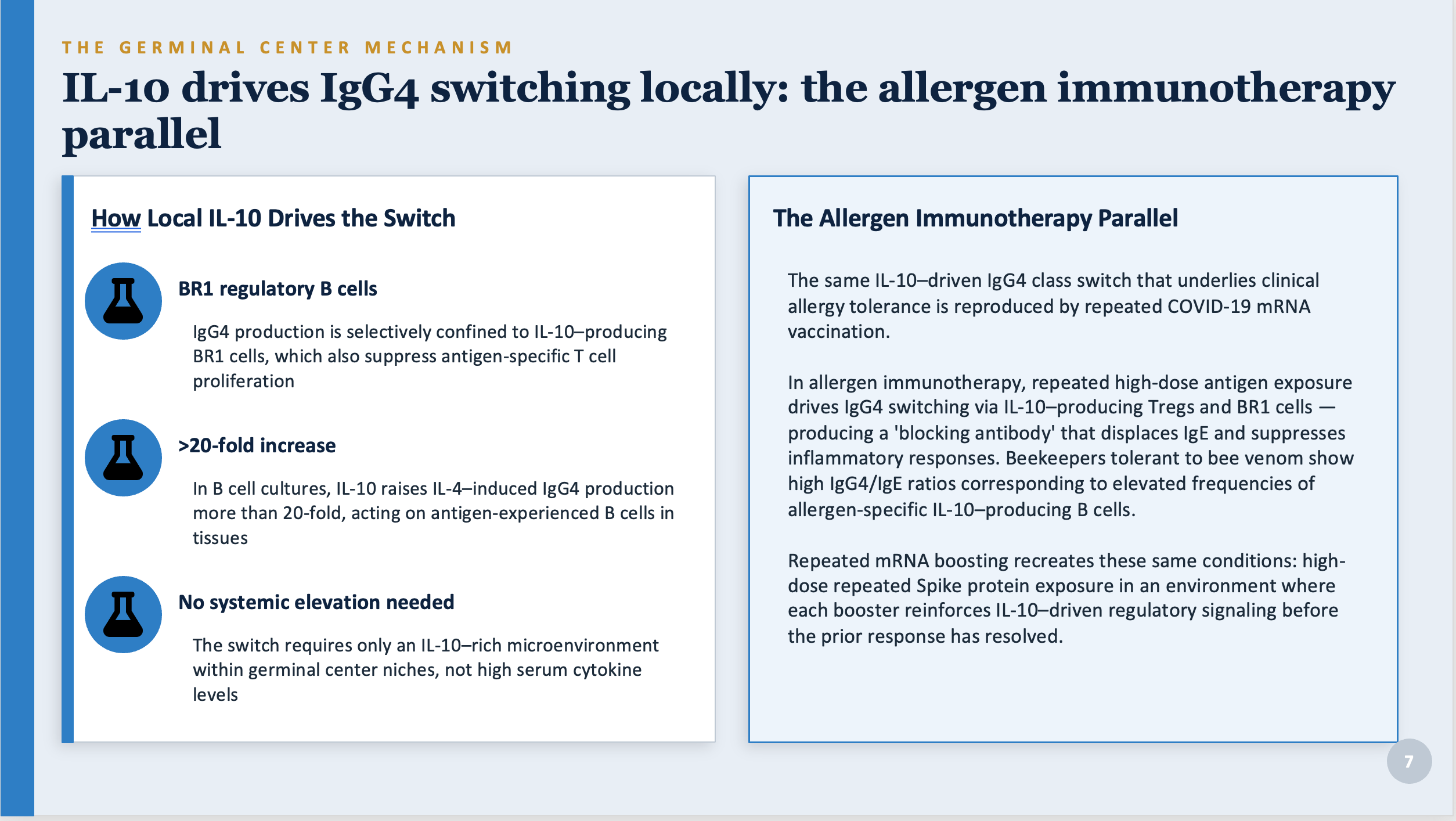
IgG4 is different. It is sometimes called the tolerance antibody. In normal life it appears in small amounts, mostly in situations where your immune system has been exposed to something repeatedly and decided it is not a threat, like bee venom in beekeepers or allergens in people completing immunotherapy. IgG4 can neutralize a virus, but it cannot perform ADCC, activate complement (another arm of the immune defense), or engage immune cell receptors that recruit other defenders to clear an infected cell.
In other words, IgG4 is a blocking antibody. It recognizes the virus and gets in the way, but it does not tell the rest of the immune system to attack.
IgG4 neutralizes the virus. It does not clear infected cells, activate complement, or recruit immune effectors. These are not equivalent things.
What repeated boosting does to that balance
After your first two COVID vaccines, your immune system produces mostly IgG1 and IgG3. The same is true after natural infection. That is the normal, expected response.
But something changes after a third dose, and in some case after the second dose, and becomes more pronounced with each additional dose. Multiple peer-reviewed studies now document that repeated mRNA boosting drives a progressive shift toward IgG4 in the antibody response specifically targeting the spike protein. This shift:
• Is not seen after natural infection alone.
• Is not seen after adenoviral vector vaccines (like AstraZeneca or Johnson & Johnson).
• Is more pronounced with the Pfizer vaccine than with Moderna.
• Has been documented in children as young as 5 after only two pediatric doses.
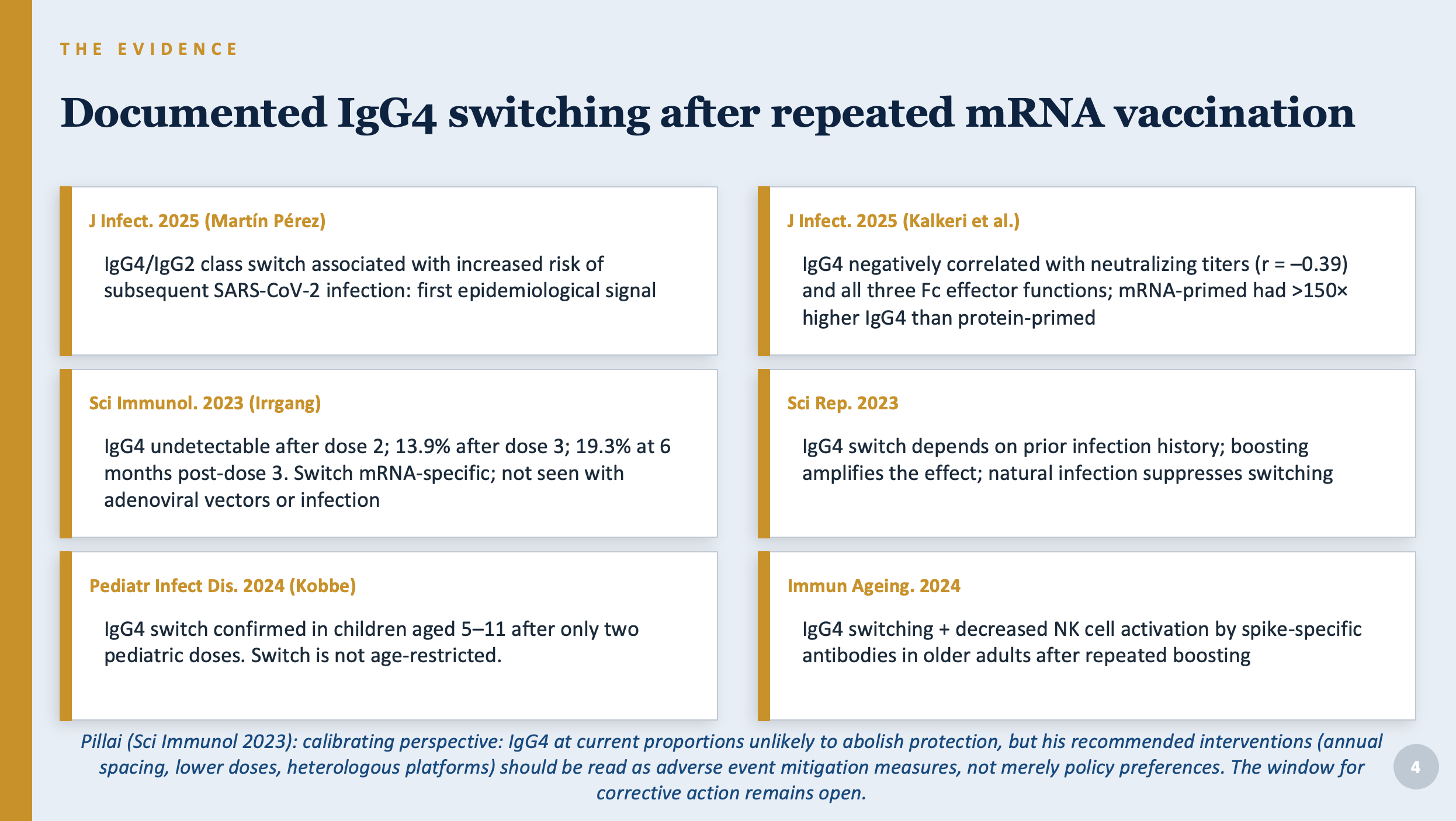
A 2025 study (Kalkeri et al., Journal of Infectious Diseases) provided the first direct functional evidence of what this switch costs. Researchers found that higher IgG4 levels were negatively correlated with the ability to neutralize the virus and with all three measured immune effector functions (the cellular and molecular processes that clear infected cells). People who had received mRNA vaccines had IgG4 levels more than 150 times higher than those who had received a protein-subunit vaccine. Note: that study was funded by Novavax, which makes a protein-subunit vaccine, and most of its authors work for Novavax. The conflict of interest is real and should be weighed. The findings are also consistent with other independent research.
A separate 2025 study (Martín Pérez et al., Journal of Infection) found that healthcare workers who developed this IgG4 shift were more likely to get subsequent COVID-19 infections. This is the first published study to associate the IgG4 switch with a real-world adverse health outcome. It requires confirmation in larger studies, but the direction of the finding is exactly what the biology predicts.
Why repeated boosting causes this shift
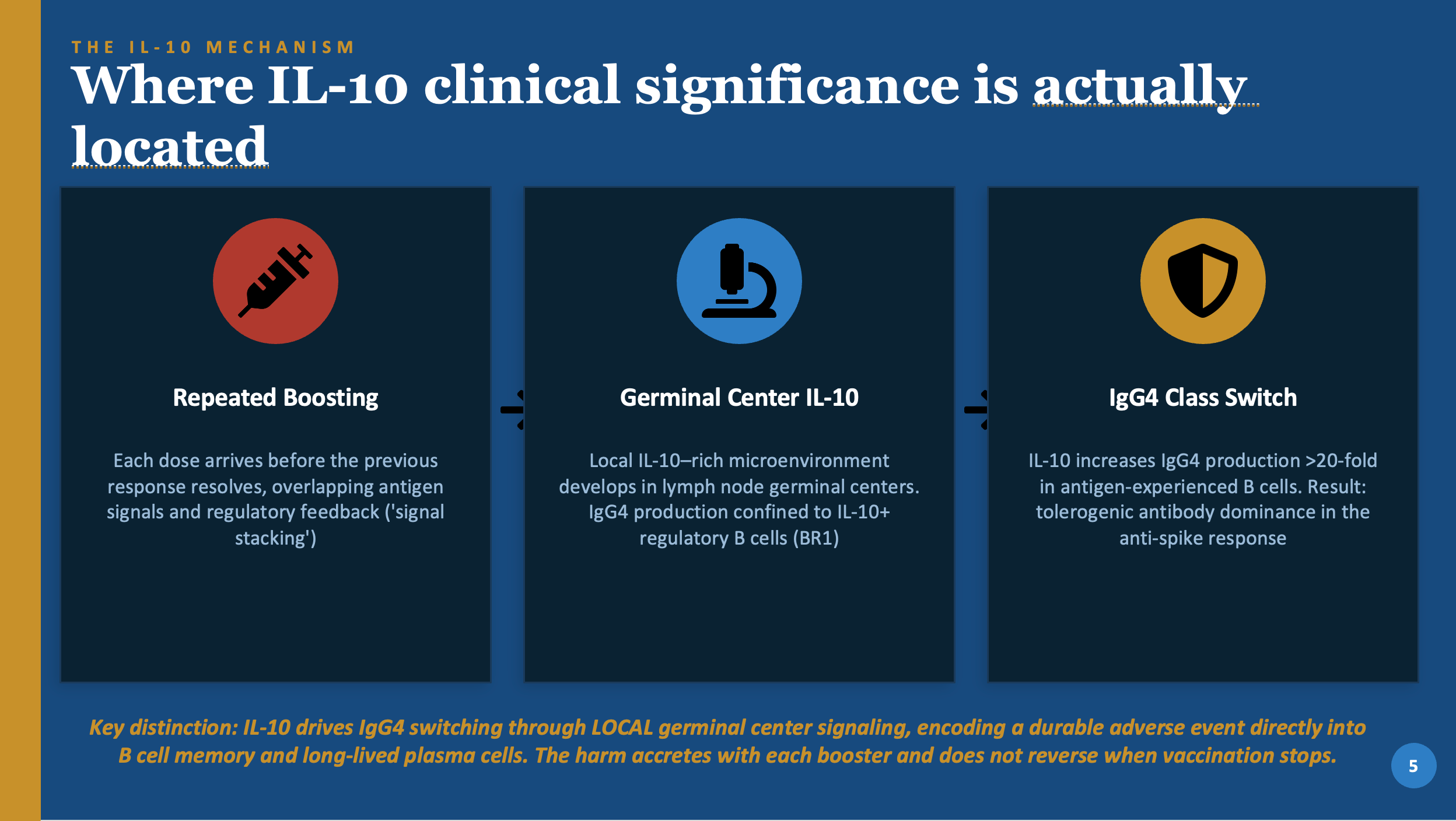
Your immune system learns from repetition. When it encounters the same antigen (in this case, the spike protein) over and over in a relatively calm context, it gradually classifies that antigen as a persistent but non-threatening presence and shifts its response toward tolerance rather than attack. This is actually a useful feature in normal life. It is the same mechanism that lets beekeepers stop reacting to bee stings and lets allergy immunotherapy work.
The shift is driven by a molecule called IL-10, a chemical signal produced inside lymph nodes during the immune response. IL-10 acts locally, in the germinal centers where new antibodies are designed and refined. When IL-10 is present in those local environments, immune cells are steered toward producing IgG4 instead of IgG1 or IgG3.
An important clarification: this is not broad immune suppression
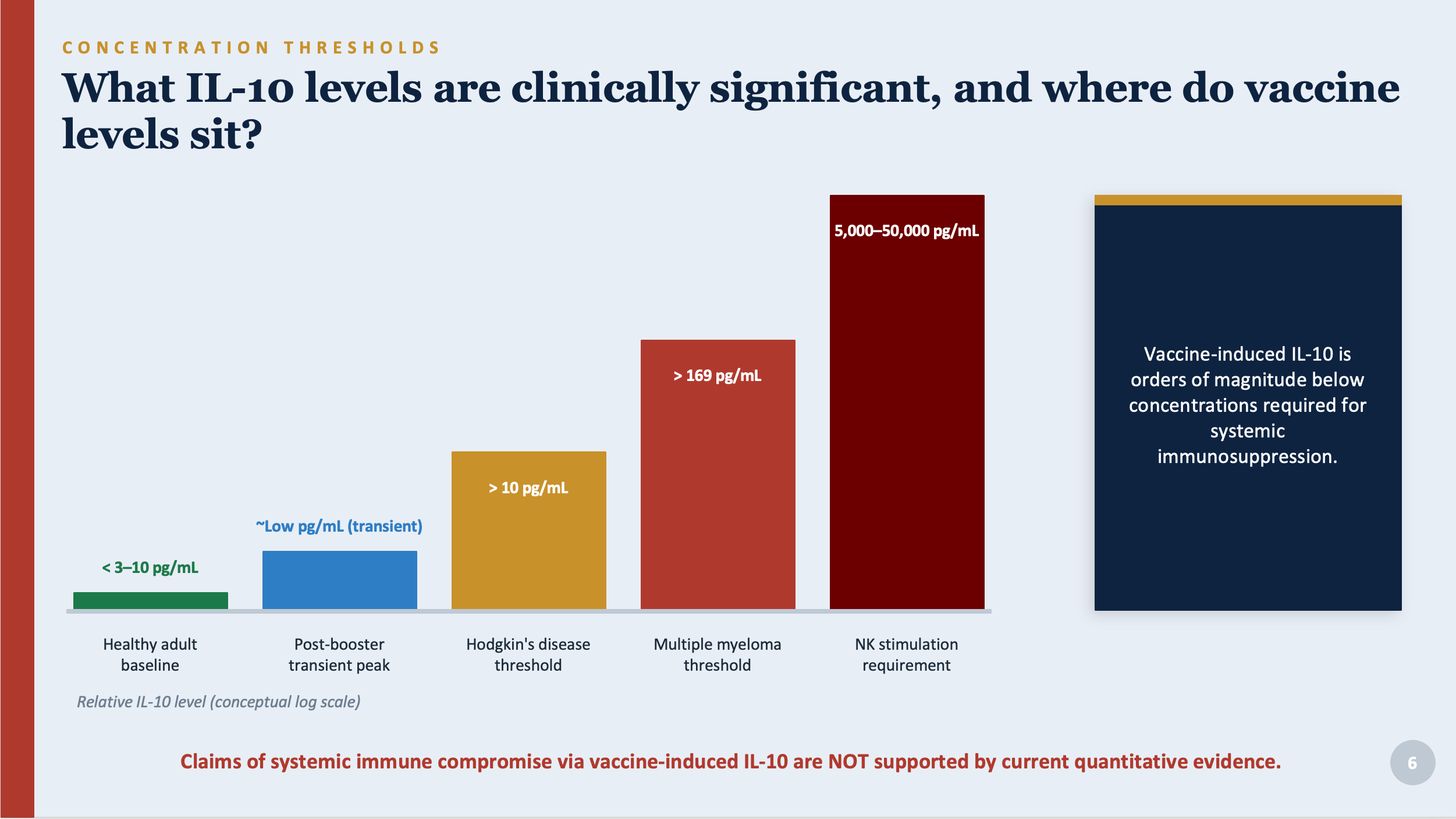
You may have read claims that COVID boosters suppress the immune system overall through elevated IL-10. This is not supported by the evidence. The quantities of IL-10 produced by vaccination are in the low picogram-per-milliliter range, tiny amounts that clear quickly. The levels required to suppress NK cells, impair T cell responses, or cause the kinds of immune dysfunction seen in cancer patients are thousands of times higher than what vaccination produces.
The real concern is not systemic immune suppression. It is a targeted, local reprogramming of the antibody production machinery inside lymph nodes. The distinction matters: broad suppression would be temporary and reversible. These local lymph node effects may impact on both immune responses to the spike antigen, as well as to other antigens being presented in the same lymph node. What the research documents is different from systemic immune suppression. It is encoded into immune memory and happens at the level of individual lymph nodes.
The memory problem
Once IgG4-producing immune cells are created in germinal centers, they take up permanent residence in bone marrow as long-lived plasma cells. They continue producing IgG4 for years. They cannot be turned off by waiting, and they are not reversed by stopping vaccination. Every subsequent encounter with the spike protein (or other antigens that have elicited similar responses in specific lymph nodes), whether from a booster or from an actual infection, triggers these cells to produce more IgG4.
Additionally, a 2024 review (Kim, Immune Networks) synthesized evidence that the mRNA-LNP vaccine platform creates unusually prolonged immune reactions in lymph nodes, lasting six months or more. This extended activity enables each booster to further engrave the IgG4 pattern into memory. The same property that makes mRNA vaccines immunologically powerful also makes them structurally prone to this effect when given frequently.
Why booster spacing matters
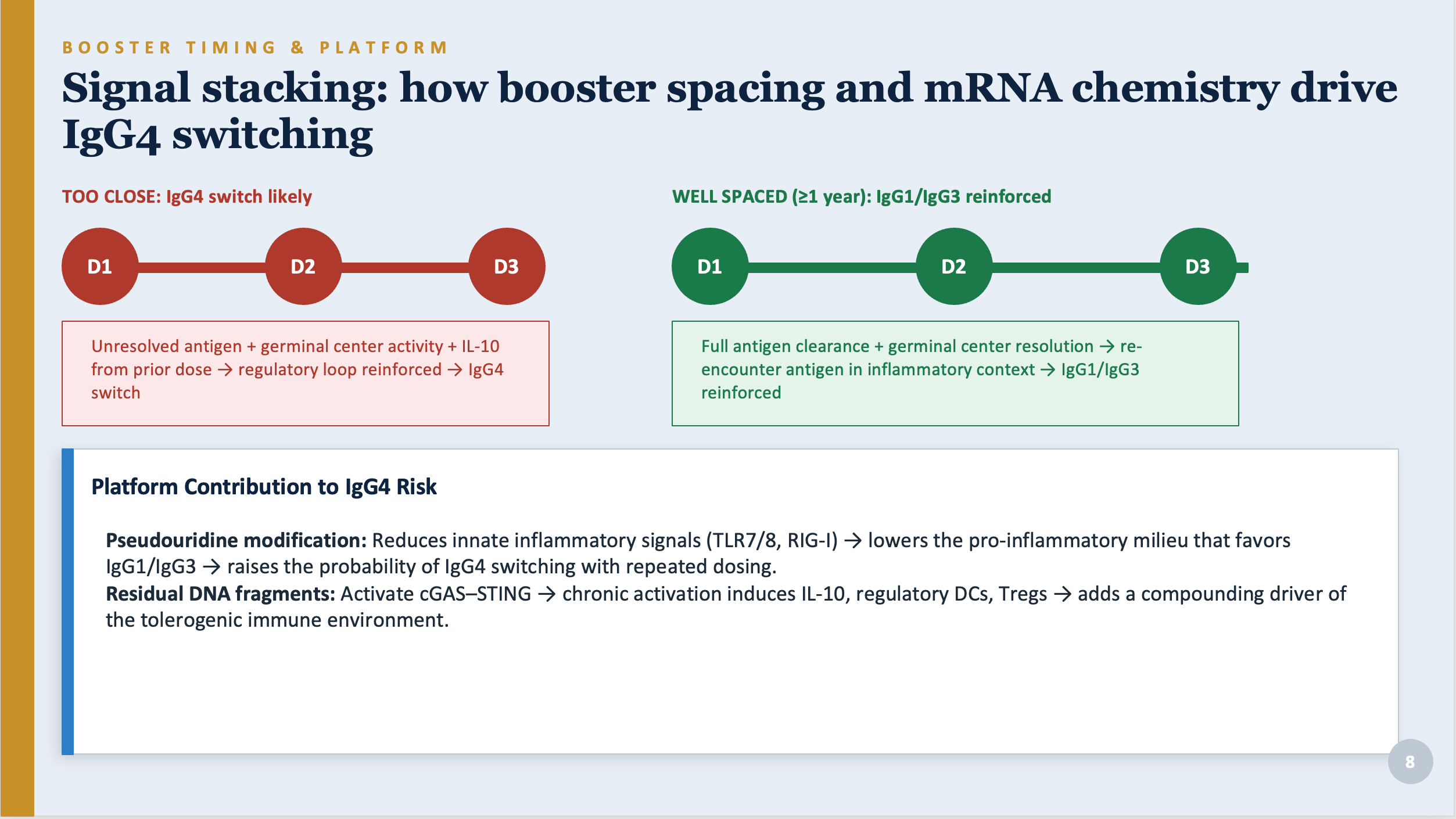
When boosters are given before the immune response to the previous dose has fully resolved, the signals overlap and amplify each other. This process is referred to as signal stacking. Each overlapping dose reinforces the IL-10 regulatory environment and pushes the IgG4 shift further. Boosters given at least a year apart allow the immune response to fully resolve and reset before re-exposure, reducing the probability of the IgG4 shift.
What the research has found: known and potential harms
This analysis divides the adverse event findings into two tiers: those documented with published evidence and those that are biologically plausible but not yet confirmed in large studies.
What is documented
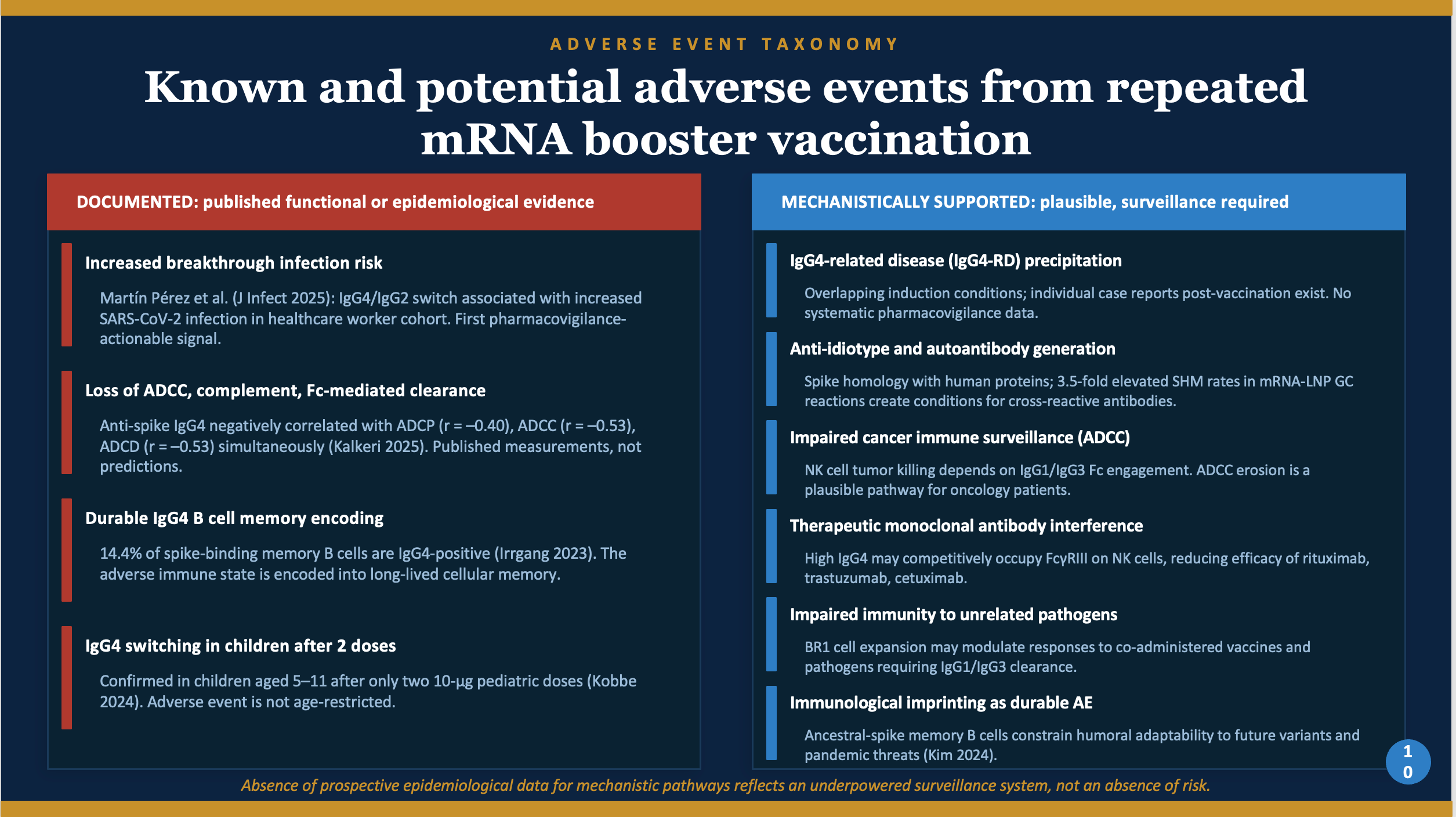
1. Increased risk of breakthrough COVID infection
Martín Pérez et al. (2025) found that healthcare workers who developed the IgG4 shift were more likely to get COVID afterward. This is the first published study to link the antibody shift to an actual adverse health outcome. It needs replication, but the direction is predicted by the biology.
2. Loss of the immune functions that clear infected cells
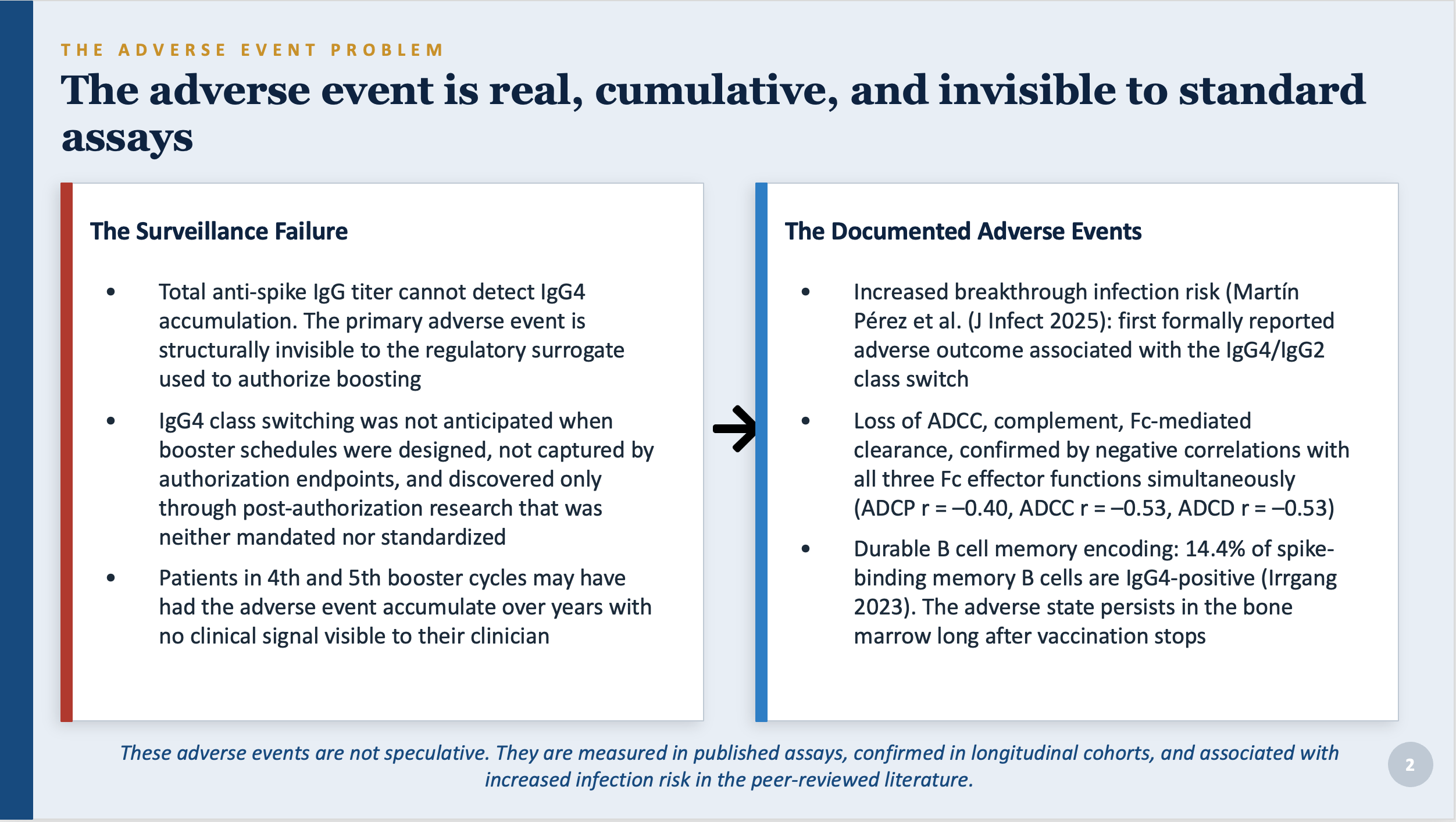
Kalkeri et al. (2025) directly measured the functional consequences. Higher IgG4 was correlated with reduced capacity for three distinct immune clearance mechanisms: ADCC (r = –0.53), complement deposition (r = –0.53), and phagocytosis (r = –0.40). These are not theories. They are published measurements.
3. The damage is written into immune memory
Irrgang et al. (Science Immunology, 2023) found that 14.4% of the long-term immune memory cells targeting the spike protein were IgG4-producing after repeated boosting. These cells persist for years. The impairment does not fade when vaccination stops.
4. Children are also affected
Kobbe et al. (Pediatric Infectious Disease Journal, 2024) confirmed IgG4 switching in children aged 5 to 11 after only two standard pediatric doses. The effect is not limited to adults who received many boosters.
What is plausible but not yet confirmed
The following risks have not been confirmed in large studies. They are raised because the biological mechanism is understood and the conditions for harm are present. Absence of confirmation here means the studies have not been done, not that the risks have been ruled out.
• IgG4-related disease (IgG4-RD). A rare inflammatory condition affecting the pancreas, kidneys, salivary glands, and other organs, driven by exactly the same immune environment that repeated boosting reinforces. Case reports of new or worsening IgG4-RD following COVID vaccination exist. No systematic surveillance has been conducted.
• Impaired cancer immune surveillance. The immune system kills early cancer cells partly through ADCC. If ADCC capacity is reduced, the body’s ability to catch and eliminate abnormal cells before they become tumors may be reduced. This is particularly relevant to patients receiving cancer immunotherapy drugs like rituximab or trastuzumab that rely on the same mechanism.
• Interference with cancer treatments. High circulating IgG4 may compete with therapeutic antibodies for the Fc receptor sites on immune cells, potentially blunting the effectiveness of ADCC-dependent cancer drugs in patients who received boosters during treatment.
• Weakened response to other vaccines and infections. The regulatory B cells expanded by repeated boosting also suppress immune responses more broadly. Whether this reduces the effectiveness of flu shots, pneumonia vaccines, or other routine immunizations given at the same time has not been studied.
• Immunological imprinting. The immune cells created by primary vaccination dominate future responses and crowd out cells that would respond to new variants. This means repeated boosters may progressively reduce your immune system’s ability to mount a fresh response to a significantly different future virus.
• Autoantibody generation. The spike protein shares structural similarities with some human proteins. The elevated mutation rates documented in mRNA-driven immune reactions create conditions for cross-reactive antibodies that might target the body’s own tissues. This has not been systematically studied.
The absence of data on these pathways does not mean they are not happening. It means no one has been looking. The surveillance system was not designed to find them.
Who this matters for, and how
The most important point in this entire paper is that the same immune shift has completely different implications depending on who you are.
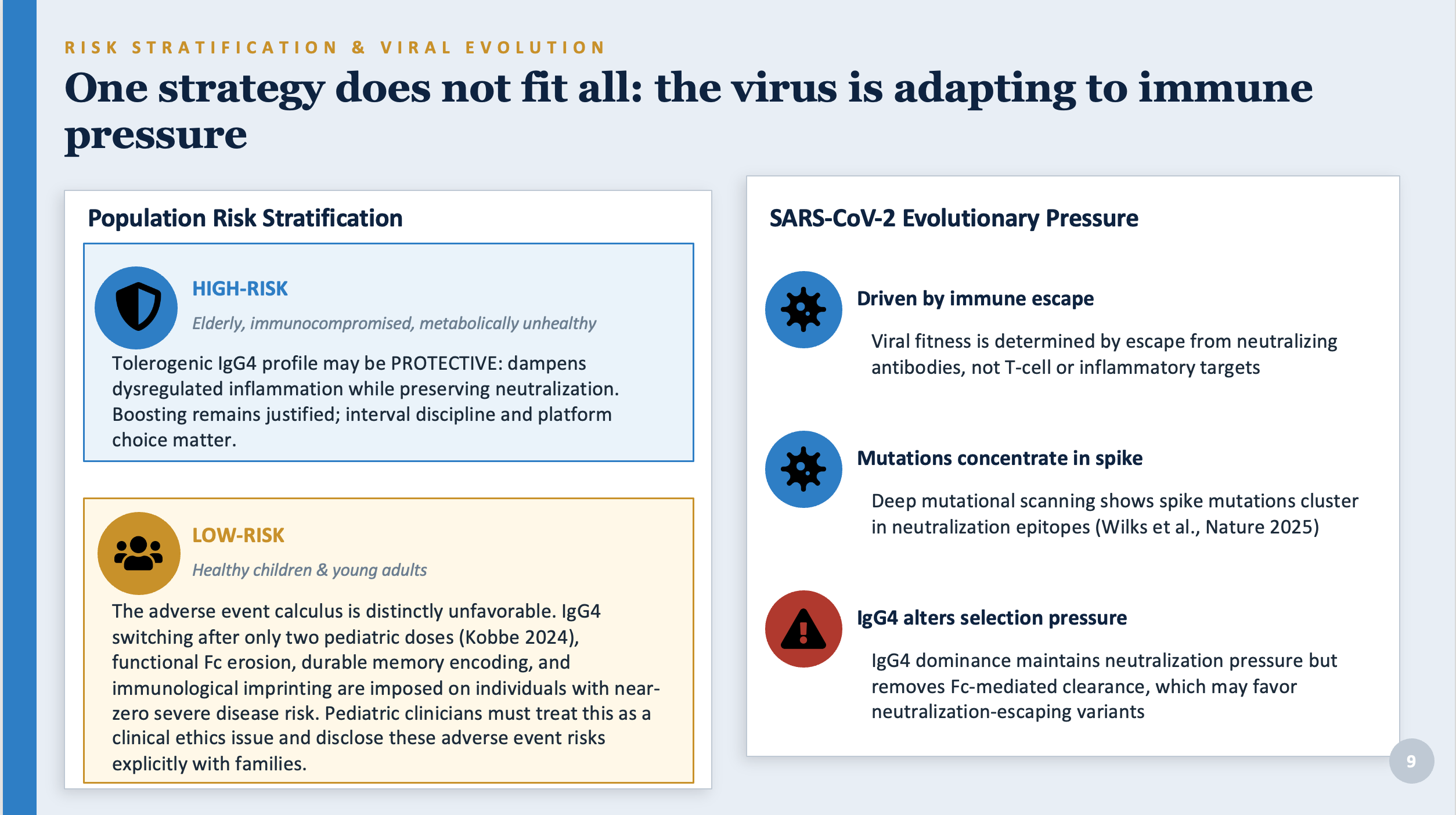
High-risk adults: elderly, immunocompromised, serious chronic illness
For people who are genuinely at high risk of severe COVID, repeated boosting is likely still the right call. COVID-19 kills primarily through excessive inflammation, not through direct viral damage. The IgG4 shift, which dampens that inflammatory response while maintaining the ability to neutralize the virus, may actually be protective for people whose biggest risk is the body’s own overreaction. The documented benefit of vaccination against severe disease and death in this group is real.
That said, even for this group, the evidence supports spacing boosters at least a year apart, considering lower doses, and possibly using a protein-subunit vaccine (like Novavax) for boosting to avoid amplifying the IgG4 shift.
Healthy adults and young people
For healthy adults who are not at elevated risk of severe COVID, the calculation is different. The individual risk of serious illness is very low. The benefits of additional boosters are small in absolute terms. And the adverse immune events documented here (loss of Fc clearance function, durable IgG4 memory encoding, immunological imprinting) are not offset by a commensurate benefit. Clinicians advising this group have an obligation to explain these trade-offs, not to present continued boosting as obviously beneficial.
Children
The findings for children are particularly concerning. Children face near-zero individual risk of severe COVID. The documented justification for vaccinating them rested almost entirely on reducing transmission to others. But the IgG4 shift produces an antibody profile that is poorly suited to preventing infection and transmission. And the shift occurs after only two standard pediatric doses, before any booster is even given.
The paper argues that pediatric clinicians should treat the question of continued boosting in healthy children as a clinical ethics issue, not a bureaucratic one. These adverse immune events are being imposed on individuals who face almost no risk of the disease being prevented, without their or their families’ informed understanding of what is happening to their immune systems.
Why your blood test cannot tell you any of this
Standard post-vaccination blood tests measure total anti-spike IgG. This number goes up after each booster. It has been used by regulatory agencies and clinicians as the primary measure of how well vaccination is working.
Total IgG titer does not distinguish between IgG1, IgG2, IgG3, and IgG4. A high number could mean you have robust protective immunity dominated by IgG1 and IgG3. It could also mean you have high antibody levels in which a substantial fraction is IgG4 and therefore cannot perform ADCC, cannot activate complement, and negatively correlates with the very neutralizing titers it is supposed to measure.
Patients who have received four or five boosters and had their antibody levels tested have no way of knowing, based on that test alone, which situation they are in. Neither do their doctors. The standard test is structurally blind to the primary adverse event.
A high antibody number after multiple boosters may reflect protection. It may also reflect a growing fraction of tolerance antibodies that actively interfere with infection clearance. The test cannot tell you which.
What needs to change
The recommendations based on this analysis are straightforward, though none of them are currently standard practice.
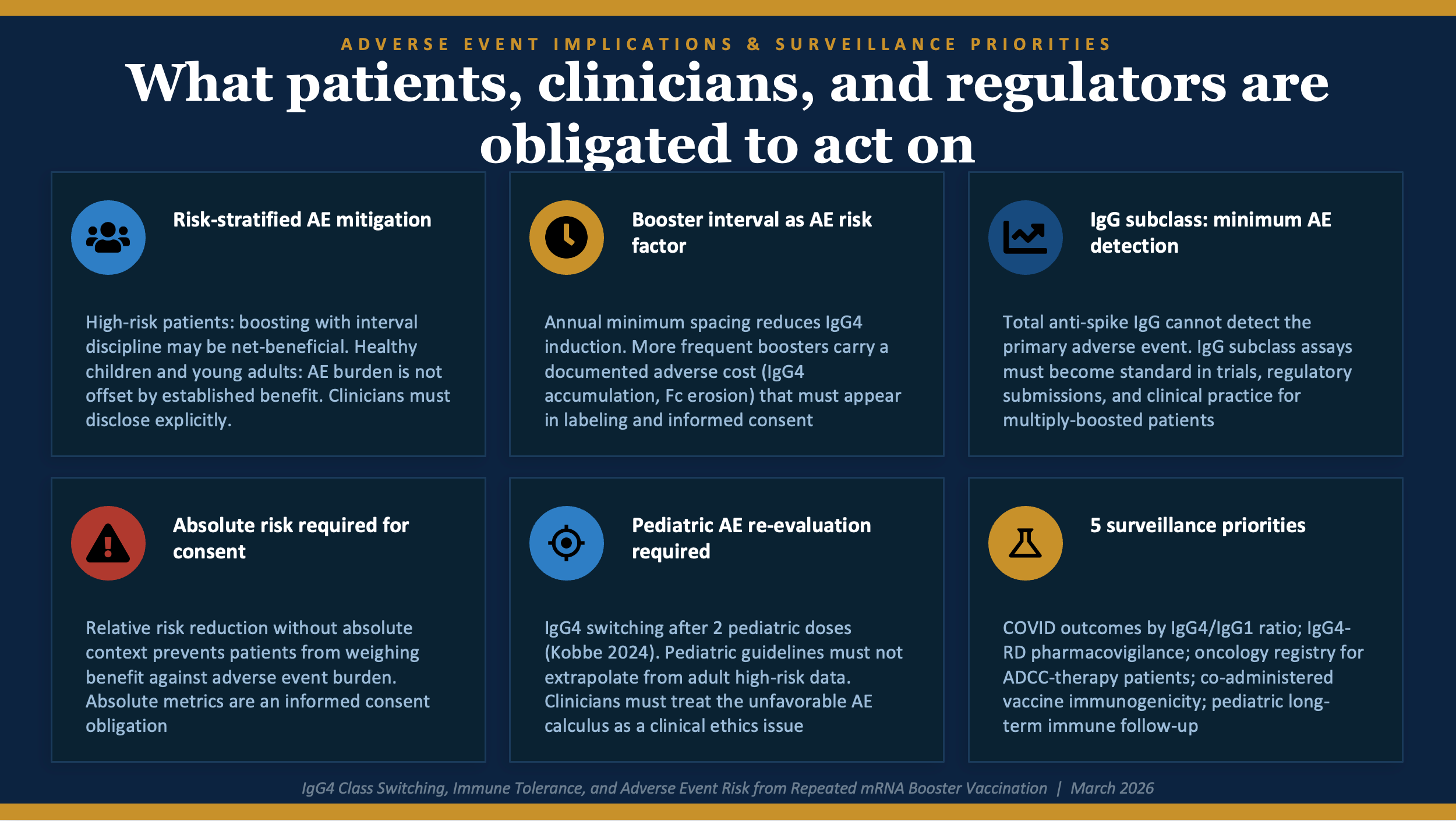
• Space boosters at least a year apart. Annual minimum intervals reduce IgG4 induction by allowing the immune response to fully resolve before re-exposure. Boosters given more frequently should be treated as carrying a known adverse cost that needs to be weighed explicitly against the benefit.
• Test for IgG subclasses, not just total IgG. Total antibody titer cannot detect the primary adverse event. IgG subclass testing should be standard in clinical trials, required by regulators before authorizing additional boosters, and available to multiply-boosted patients who want to know what kind of antibody response they actually have.
• Use absolute, not relative, risk numbers. Patients deserve to know how much a booster actually reduces their absolute risk of infection, not just what percentage improvement it produces relative to an unspecified baseline. Relative risk numbers without absolute context make small benefits appear large and prevent meaningful weighing of benefit against harm.
• Re-evaluate pediatric booster policy with new data. Pediatric booster guidelines should not be derived by scaling down adult high-risk recommendations. Children need their own evidence base, with IgG subclass outcomes measured, before continued boosting is recommended as standard care.
• Start the surveillance studies that should have been started years ago. At minimum: prospective studies measuring COVID outcomes by IgG subclass composition; review of IgG4-related disease cases linked to vaccination; studies of outcomes in cancer patients on ADCC-dependent therapies who also received boosters; and long-term immune follow-up in children.
• Clinicians must disclose these trade-offs. Patients who received multiple boosters under the understanding that more was always better deserve an accurate accounting of what the immunological evidence now shows. That is what informed consent means.
The bottom line
The current data indicate that COVID-19 mRNA vaccines work for reducing the incidence of severe disease and death in high-risk patients. They have prevented serious illness and death in many people who were genuinely at risk. That is not being disputed in this analysis. Whether the risk/benefit analysis is positive for these products for any cohort is another matter entirely, and not being addressed in this analysis.
What is under dispute is whether repeated boosting is uniformly beneficial across all populations, whether the antibody tests used to justify it measure what matters, and whether the people receiving these boosters have been given an accurate picture of what is happening to their immune systems.
The answer to all three questions is no. The immune shift documented in this research is real, it has measurable functional consequences, it compounds with each additional booster, it is invisible to standard testing, and its long-term effects are unknown because the studies needed to characterize them have not been done.
None of that requires catastrophic projections or “conspiracy theories”. It does require honesty.
The question is not whether the vaccines worked. The question is whether we understood what we were doing to the immune systems of tens of millions of people, and whether we are willing to find out now.
Dr. Malone. It's articles like these that first convinced me to sign up to your substack. These plain English guides explaining what really happens after taking the mRNA vax and boosters are invaluable for everyday people that want to understand the risks and consequences that their doctors and the mainstream media never mention. It infuriates me when I see how the media, and even some of your peers vilify you. Thank you for all you do!
I had a sister in law that received Covid vaccines and EVERY booster offered. She was terrified of the disease and never left her home during the initial "outbreak". She developed ovarian cancer in Feb 2022 , Stage 3C initially. She underwent Neoadjuvant chemo, followed by surgery, then chemo again, then immunotherapy with oral Lynparza. All standardized treatments. She did well for 20 months, which is a great response, but then PET scan showed a very small recurrence in the pelvic region, which is a normal recurrence, especially for Stage 3 C. She began chemo again per NCCN guidelines, but this time ( as she continued getting every booster ) her body rejected EVERY treatment drug offered, even the same drugs given previously with success. Sadly after exhausting all drug options, even targeted therapies based on genetic mutations, she passed away last year. Although I know Stage 3C is hard to overcome, I have witnessed ( I am a retired Oncology RN) many older patients and sicker with chronic disease patients overcome this stage successfully , but they either did not receive Covid injections initially, only got one or two injections or did not continue to get the multiple Boosters. I without a doubt blame the vaccine and the multiple boosters on her demise....and of course the media for the propoganda that led her to make these decisions. For the record, she was a (supposedly) well educated person.